You might also like
- Regulatory AffairsDocument39 pagesRegulatory Affairssivaram888100% (2)
- Community Pharmacy Survey ToolDocument3 pagesCommunity Pharmacy Survey ToolEarl Cedric DL DalmacioNo ratings yet
- Drug Registration in ASEAN CountriesDocument35 pagesDrug Registration in ASEAN CountriesSreedhar TirunagariNo ratings yet
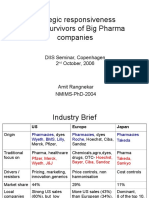
- Global Pharma StrategyDocument15 pagesGlobal Pharma StrategyDr Amit RangnekarNo ratings yet
- Pharmacy Orientation ProgramDocument48 pagesPharmacy Orientation ProgramShardendu MishraNo ratings yet
- RosuNext (Market Plan For PPI)Document15 pagesRosuNext (Market Plan For PPI)Muhammad UmerNo ratings yet
- Manual For Medicines Good DispensingDocument114 pagesManual For Medicines Good DispensingJosh SorianoNo ratings yet
- NUP ManifestoDocument47 pagesNUP ManifestoAfrican Centre for Media Excellence100% (1)
- Nepalese Pharmaceutical Industries & Who GMPDocument6 pagesNepalese Pharmaceutical Industries & Who GMPJaya Bir Karmacharya100% (1)
- RANBAXYDocument76 pagesRANBAXYRickyMartynNo ratings yet
- Pharmacy SOPDocument86 pagesPharmacy SOPAlyNo ratings yet
- Kabuleta Kiiza Joseph ManifestoDocument27 pagesKabuleta Kiiza Joseph ManifestoAfrican Centre for Media ExcellenceNo ratings yet
- Pharma Business Dynamics in ROW MarketsDocument9 pagesPharma Business Dynamics in ROW Marketskaushal_75No ratings yet
- Edited KSDP FinalDocument55 pagesEdited KSDP Finalathiraskumar4750% (2)
- Absa Africa Financial Market IndexDocument40 pagesAbsa Africa Financial Market IndexSandraNo ratings yet
- Pharmaceutical Wholesaler Checklist 2 0Document16 pagesPharmaceutical Wholesaler Checklist 2 0atulbs100% (2)
- Law State Board of PharmacyDocument5 pagesLaw State Board of Pharmacyeze24No ratings yet
- National Pharmaceutical Master PlanDocument13 pagesNational Pharmaceutical Master PlanNitu AhmadNo ratings yet
- Requirements To Establish A Retail Pharmacy Business 1Document5 pagesRequirements To Establish A Retail Pharmacy Business 1Allan Alejandro Sevilla IINo ratings yet
- Pharmaceuticals Executive SummaryDocument10 pagesPharmaceuticals Executive SummaryPradyot78No ratings yet
- Leadership Essentials of PharmacistDocument15 pagesLeadership Essentials of PharmacistMuzammil Shaikh Bismil100% (1)
- Pharmacy: Undergraduate Study 2016Document18 pagesPharmacy: Undergraduate Study 2016kgiyerNo ratings yet
- 3 Puntland Health Policy FrameworkDocument46 pages3 Puntland Health Policy Frameworkkunciil100% (1)
- Pharmacy Practice Guidance Manual - IrelandDocument62 pagesPharmacy Practice Guidance Manual - IrelandTim Lai100% (1)
- Pharmaceutical Marketing Case StudyDocument8 pagesPharmaceutical Marketing Case StudyMd. Nure Alamin SiddikNo ratings yet
- Establishment of Drug Information CentreDocument15 pagesEstablishment of Drug Information CentreSherry Abdel Hakam50% (2)
- Project Report On Pharmaceutical Unit (Tablet, Capsules, Syrups, Ointments, Lotion, Nebulizer)Document16 pagesProject Report On Pharmaceutical Unit (Tablet, Capsules, Syrups, Ointments, Lotion, Nebulizer)EIRI Board of Consultants and PublishersNo ratings yet
- Business ProposalDocument13 pagesBusiness ProposalPrapti Bhatt0% (1)
- Ham Enterprises LTD V DTB - Case CommentDocument11 pagesHam Enterprises LTD V DTB - Case CommentAfrican Centre for Media Excellence100% (1)
- Oral Controlled Release Formulation Design and Drug Delivery: Theory to PracticeFrom EverandOral Controlled Release Formulation Design and Drug Delivery: Theory to PracticeHong WenNo ratings yet
- Lupin Pharmaceutical Corporate StrategyDocument53 pagesLupin Pharmaceutical Corporate Strategyhagar sudhaNo ratings yet
- Pharmd Programme Handbook Faculty of Medical Sciences Entry Level Doctor of Pharmacy PDFDocument53 pagesPharmd Programme Handbook Faculty of Medical Sciences Entry Level Doctor of Pharmacy PDFJmv Velazquez100% (1)
- 2011 The Pharmaceutical Industry and Global HealthDocument50 pages2011 The Pharmaceutical Industry and Global HealthAbe GuinigundoNo ratings yet
- Community Pharmacy Planning To Open A Retail Pharmacy Launching A New Pharmacy Physical Environment of A Retail PharmacyDocument13 pagesCommunity Pharmacy Planning To Open A Retail Pharmacy Launching A New Pharmacy Physical Environment of A Retail PharmacySanam BangashNo ratings yet
- Drug Information CentersDocument11 pagesDrug Information CentersAbid Ali Khan57% (7)
- Requirements For Drug Information CentresDocument5 pagesRequirements For Drug Information CentresDara Kurnia JatiNo ratings yet
- Daily Monitor Sexual Harassment PolicyDocument11 pagesDaily Monitor Sexual Harassment PolicyAfrican Centre for Media ExcellenceNo ratings yet
- Presentation Marketing and Distribution ChannelsDocument15 pagesPresentation Marketing and Distribution Channelsavtarsingsadaf_28176No ratings yet
- The Global Pharmaceutical IndustryDocument15 pagesThe Global Pharmaceutical IndustryKia LadnomNo ratings yet
- UGANDA Voter Count by Polling Stations 2021Document1,446 pagesUGANDA Voter Count by Polling Stations 2021jadwongscribdNo ratings yet
- Journal of Learning InsightsDocument12 pagesJournal of Learning InsightsJisel-Apple Bulan100% (2)
- Pharmacy Practice in Developing Countries: Achievements and ChallengesFrom EverandPharmacy Practice in Developing Countries: Achievements and ChallengesNo ratings yet
- Analysis of The Pharmaceutical IndustryDocument69 pagesAnalysis of The Pharmaceutical Industrymohammed_jibran67% (3)
- High Risk Medication PolicyDocument44 pagesHigh Risk Medication PolicyDewi Ratna SariNo ratings yet
- Contract For Pharmacists EODocument10 pagesContract For Pharmacists EODavid Oba-Ogoh Dushie0% (1)
- How Telecom Operators in Africa Are Failing Persons With DisabilitiesDocument23 pagesHow Telecom Operators in Africa Are Failing Persons With DisabilitiesAfrican Centre for Media ExcellenceNo ratings yet
- Isoniazid Preventive Therapy in UgandaDocument27 pagesIsoniazid Preventive Therapy in UgandaNsubugaNo ratings yet
- PEST Analysis of Pharmaceutical Industry of BangladeshDocument11 pagesPEST Analysis of Pharmaceutical Industry of BangladeshEkjon Dipto100% (2)
- COPPDocument1 pageCOPPYogesh ChaudhariNo ratings yet
- Self-Medication Practices Among ResidentDocument4 pagesSelf-Medication Practices Among ResidentSyed Shabbir HaiderNo ratings yet
- Risk in Pharma SectorDocument29 pagesRisk in Pharma SectorRajesh Basanna100% (2)
- Ethiopian Pharmaceutical Industry-1st DraftDocument15 pagesEthiopian Pharmaceutical Industry-1st Draftzerayakob88% (8)
- Community Pharmacy Layout Full ChapterDocument4 pagesCommunity Pharmacy Layout Full ChaptersaleemNo ratings yet
- Registration Procedure of Marketing Authorization of Medicinal Product in MalaysiaDocument17 pagesRegistration Procedure of Marketing Authorization of Medicinal Product in MalaysiaFitrah Zulfikar MansyurNo ratings yet
- Pharma Industry: Vipul Murarka Vibhuti SharmaDocument37 pagesPharma Industry: Vipul Murarka Vibhuti SharmaVipul MurarkaNo ratings yet
- Ethiopia PharmaceuticalDocument44 pagesEthiopia PharmaceuticalLydia Tujuba AtomssaNo ratings yet
- Square PharmaDocument2 pagesSquare PharmaJobaiyer AlamNo ratings yet
- Assignment - Beximco Pharmaceuticals Bangladesh LimitedDocument14 pagesAssignment - Beximco Pharmaceuticals Bangladesh LimitedAhmad O. ShakurNo ratings yet
- Pharmaceutical Industry of PakistanDocument20 pagesPharmaceutical Industry of PakistanAli UsamaNo ratings yet
- Pharmaceutical IndustryDocument34 pagesPharmaceutical Industryalizain8000% (1)
- 10-K WalgreensDocument366 pages10-K Walgreensroger DoddNo ratings yet
- Jan Aushadhi Scheme New BusinessplanDocument36 pagesJan Aushadhi Scheme New BusinessplaniddrxNo ratings yet
- Pharmaceutical IndustryDocument18 pagesPharmaceutical IndustryKrishna PrasadNo ratings yet
- Ethics in Pharmaceutical Industry PDFDocument2 pagesEthics in Pharmaceutical Industry PDFMichelle0% (1)
- General Profile of The CompanyDocument25 pagesGeneral Profile of The Companyapi-235704876No ratings yet
- Pharmaceutical LicensingDocument13 pagesPharmaceutical Licensingkumari astha rupaliNo ratings yet
- FDA AlertDocument2 pagesFDA AlertAnonymous Pb39klJNo ratings yet
- Community PharmacyDocument8 pagesCommunity PharmacyAmit KumarNo ratings yet
- Pharmacy ActDocument32 pagesPharmacy ActAditya Varshneya100% (1)
- National Guidelines For Management of Covid-19Document203 pagesNational Guidelines For Management of Covid-19African Centre for Media ExcellenceNo ratings yet
- STG BabyDocument464 pagesSTG BabyXaveeNo ratings yet
- National Guidelines For Management of Covid-19Document203 pagesNational Guidelines For Management of Covid-19African Centre for Media ExcellenceNo ratings yet
- Economic Performance Report, June 2021Document39 pagesEconomic Performance Report, June 2021African Centre for Media ExcellenceNo ratings yet
- Rejoinder Statement by Amelia Kyambadde To ParliamentDocument4 pagesRejoinder Statement by Amelia Kyambadde To ParliamentAfrican Centre for Media ExcellenceNo ratings yet
- Vision Group Sexual Harassment PolicyDocument4 pagesVision Group Sexual Harassment PolicyAfrican Centre for Media ExcellenceNo ratings yet
- Presidential Election PetitionDocument14 pagesPresidential Election PetitionAfrican Centre for Media ExcellenceNo ratings yet
- Editors Guild CEPIL V AG MC 400 of 2020Document10 pagesEditors Guild CEPIL V AG MC 400 of 2020African Centre for Media ExcellenceNo ratings yet
- Cabinet DecisionsDocument6 pagesCabinet DecisionsAfrican Centre for Media ExcellenceNo ratings yet
- Report of Budget Committee On Supplementary ExpenditureDocument33 pagesReport of Budget Committee On Supplementary ExpenditureAfrican Centre for Media ExcellenceNo ratings yet
- Amended Presidential Election PetitionDocument28 pagesAmended Presidential Election PetitionAfrican Centre for Media ExcellenceNo ratings yet
- Elected Members of Parliament 2021Document13 pagesElected Members of Parliament 2021African Centre for Media Excellence100% (2)
- NRM Manifesto 2021-2026Document376 pagesNRM Manifesto 2021-2026African Centre for Media ExcellenceNo ratings yet
- Tumukunde ManifestoDocument20 pagesTumukunde ManifestoAfrican Centre for Media ExcellenceNo ratings yet
- Uganda Media Coverage of The 2021 Elections - December 2020Document86 pagesUganda Media Coverage of The 2021 Elections - December 2020African Centre for Media ExcellenceNo ratings yet
- Voter Count by District 2021Document4 pagesVoter Count by District 2021African Centre for Media ExcellenceNo ratings yet
- Alliance For National Transformation ManifestoDocument50 pagesAlliance For National Transformation ManifestoAfrican Centre for Media ExcellenceNo ratings yet
- Pastor Fred Mwesigye ManifestoDocument24 pagesPastor Fred Mwesigye ManifestoAfrican Centre for Media ExcellenceNo ratings yet
- Nancy Linda Kalembe ManifestoDocument14 pagesNancy Linda Kalembe ManifestoAfrican Centre for Media ExcellenceNo ratings yet
- FDC ManifestoDocument70 pagesFDC ManifestoAfrican Centre for Media ExcellenceNo ratings yet
- National Election Watch-Uganda Statement On NRM Primary ElectionsDocument12 pagesNational Election Watch-Uganda Statement On NRM Primary ElectionsAfrican Centre for Media ExcellenceNo ratings yet
- NRM Manifesto 2021-2026Document288 pagesNRM Manifesto 2021-2026African Centre for Media ExcellenceNo ratings yet
- Monetary Policy Statement October 2020Document2 pagesMonetary Policy Statement October 2020African Centre for Media ExcellenceNo ratings yet
- Data Protection and Privacy Regulations, 2020Document36 pagesData Protection and Privacy Regulations, 2020African Centre for Media ExcellenceNo ratings yet
- State of The Economy September 2020Document33 pagesState of The Economy September 2020African Centre for Media ExcellenceNo ratings yet
- Pineda and Llamo Cases - FornesteDocument15 pagesPineda and Llamo Cases - FornesteIrish Claire FornesteNo ratings yet
- Asco Anzsco One To One CorrelationsDocument10 pagesAsco Anzsco One To One CorrelationsNirosh AmadorugeNo ratings yet
- CV Muzaffar MahaDocument8 pagesCV Muzaffar Mahaapi-665372449No ratings yet
- Application Form For Employment in EchsDocument4 pagesApplication Form For Employment in EchssnehalrajNo ratings yet
- Pharmacy P&PDocument394 pagesPharmacy P&PzeljenNo ratings yet
- Stefan Nickolas OurlianDocument4 pagesStefan Nickolas OurlianJames LindonNo ratings yet
- Guidelines For Registration of Pharmaceutical Premises in Nigeria by Pharm Saidu BurjiDocument10 pagesGuidelines For Registration of Pharmaceutical Premises in Nigeria by Pharm Saidu BurjiYPS NetworkNo ratings yet
- Fact Sheet 1 - More About The GPHCDocument2 pagesFact Sheet 1 - More About The GPHCGeneral Pharmaceutical CouncilNo ratings yet
- Pharm 213 - Unit 2Document3 pagesPharm 213 - Unit 2Nics De GraciaNo ratings yet
- Foundations of Professional NursingDocument41 pagesFoundations of Professional Nursingnb6pd5rvnxNo ratings yet
- Community PharmacyDocument90 pagesCommunity Pharmacyadili soohaaNo ratings yet
- Health Sector in Ghana ReviewDocument17 pagesHealth Sector in Ghana ReviewBriant BlantonNo ratings yet
- Code+of+Ethics OCPDocument2 pagesCode+of+Ethics OCPZoher HalaiNo ratings yet
- Hospital Pharmacy Practice in Saudi Arabia: Dispensing and Administration in The Riyadh RegionDocument9 pagesHospital Pharmacy Practice in Saudi Arabia: Dispensing and Administration in The Riyadh RegionNisa SundariNo ratings yet
- Code of Conduct For Pharmacy StudentsDocument12 pagesCode of Conduct For Pharmacy StudentsmysaddreamNo ratings yet
- Hospital Formulart PPT NotesDocument16 pagesHospital Formulart PPT NotesAbhijith A pNo ratings yet
- Career Overview: Ajith VasudevanDocument3 pagesCareer Overview: Ajith Vasudevanmohamed sewilamNo ratings yet
- Mercury Drug Corp Vs de LeonDocument13 pagesMercury Drug Corp Vs de LeonJuan TañamorNo ratings yet
- Research in Social and Administrative PharmacyDocument7 pagesResearch in Social and Administrative PharmacymuftiaNo ratings yet
- Shri Govindram Seksaria Institute of Technology and ScienceDocument33 pagesShri Govindram Seksaria Institute of Technology and ScienceSunny Thakur17No ratings yet
- The Nine-Star Pharmacist: An Overview: Aaseer Thamby Sam and Subramani ParasuramanDocument4 pagesThe Nine-Star Pharmacist: An Overview: Aaseer Thamby Sam and Subramani ParasuramanErlia Anggrainy SianiparNo ratings yet
- EP SPass Form8Document15 pagesEP SPass Form8Harold PanesNo ratings yet
- Lincy Varughese CVDocument8 pagesLincy Varughese CVapi-302147754No ratings yet
- 1) Community PharmacyDocument17 pages1) Community PharmacyDr. Zirwa AsimNo ratings yet