You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Relationships, 365 Day Devotional Mylesunroe 377pgDocument377 pagesRelationships, 365 Day Devotional Mylesunroe 377pgEla100% (7)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unofficial Aterlife GuideDocument33 pagesThe Unofficial Aterlife GuideIsrael Teixeira de AndradeNo ratings yet
- Viscous Fluid Flow Frank M White Third Edition - Compress PDFDocument4 pagesViscous Fluid Flow Frank M White Third Edition - Compress PDFDenielNo ratings yet
- Assignment 4 SolutionsDocument9 pagesAssignment 4 SolutionsNengke Lin100% (2)
- Active Faults in MalaysiaDocument52 pagesActive Faults in MalaysiaHazim HaNo ratings yet
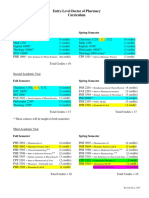
- Pharmd CurriculumDocument18 pagesPharmd Curriculum5377773No ratings yet
- Chapter 1 (PLC)Document9 pagesChapter 1 (PLC)Kibria PrangonNo ratings yet
- SPM 1449 2006 Mathematics p2 BerjawapanDocument18 pagesSPM 1449 2006 Mathematics p2 Berjawapanpss smk selandar71% (7)
- Tuesday, 16 November 2021 - Afternoon Discovering ElectronicsDocument20 pagesTuesday, 16 November 2021 - Afternoon Discovering Electronicsnvmalt070No ratings yet
- Disectie AnatomieDocument908 pagesDisectie AnatomieMircea SimionNo ratings yet
- Table 1 Minimum Separation DistancesDocument123 pagesTable 1 Minimum Separation DistancesjhonNo ratings yet
- Simple Roll-Type: A Loud SpeakerDocument1 pageSimple Roll-Type: A Loud SpeakerEudes SilvaNo ratings yet
- Frontinus - Water Management of RomeDocument68 pagesFrontinus - Water Management of RomezElfmanNo ratings yet
- American University of BeirutDocument21 pagesAmerican University of BeirutWomens Program AssosciationNo ratings yet
- c083c282a43655ec69532f2704c3993aDocument12 pagesc083c282a43655ec69532f2704c3993aAneilRandyRamdialNo ratings yet
- The Wild T1 TheodoliteDocument61 pagesThe Wild T1 TheodoliteCJLara100% (1)
- Product Stock Exchange Learn BookDocument1 pageProduct Stock Exchange Learn BookSujit MauryaNo ratings yet
- Earth Science (Metamorphic Rocks)Document8 pagesEarth Science (Metamorphic Rocks)MA. ALEXIS LAURENNo ratings yet
- Crashing Is A Schedule Compression Technique Used To Reduce or Shorten The Project ScheduleDocument1 pageCrashing Is A Schedule Compression Technique Used To Reduce or Shorten The Project ScheduleRaymart BulagsacNo ratings yet
- Manufacuring EngineeringDocument3 pagesManufacuring Engineeringapi-79207659No ratings yet
- Me8072 Renewable Sources of EnergyDocument13 pagesMe8072 Renewable Sources of EnergyNallappan Rajj ANo ratings yet
- Zincanode 304 pc142Document3 pagesZincanode 304 pc142kushar_geoNo ratings yet
- Earth Sciences Notes Csir-Ugc Net JRFDocument57 pagesEarth Sciences Notes Csir-Ugc Net JRFmanas773No ratings yet
- Final TestDocument10 pagesFinal TestbennyNo ratings yet
- RhythmDocument10 pagesRhythmSalcedo NoelNo ratings yet
- Easergy PS100 48VDC Power SupplyDocument2 pagesEasergy PS100 48VDC Power SupplyRichard SyNo ratings yet
- Generalized Anxiety DisorderDocument24 pagesGeneralized Anxiety DisorderEula Angelica OcoNo ratings yet
- LighthouseDocument4 pagesLighthousejaneborn5345No ratings yet
- Relationsh Between EM and Young S ModuliDocument7 pagesRelationsh Between EM and Young S ModuliDwight AndersonNo ratings yet