You might also like
- Lab Values Chart GuideDocument5 pagesLab Values Chart GuideVanessaMUeller100% (3)
- Physical Assessment ChartDocument1 pagePhysical Assessment ChartVanessaMUellerNo ratings yet
- Alcohol Withdrawal Care PlanDocument1 pageAlcohol Withdrawal Care PlanVanessaMUellerNo ratings yet
- Example 1 - Focus: Nausea Related To AnestheticDocument1 pageExample 1 - Focus: Nausea Related To AnestheticVanessaMUellerNo ratings yet
- Penuemonia Care PalnDocument2 pagesPenuemonia Care PalnVanessaMUellerNo ratings yet
- Name Age Room Code Dr. Isolation Activity Diet Allergy: DX: HXDocument1 pageName Age Room Code Dr. Isolation Activity Diet Allergy: DX: HXVanessaMUellerNo ratings yet
- Updated Clinical SheetDocument1 pageUpdated Clinical SheetVanessaMUellerNo ratings yet
- Fluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitDocument1 pageFluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitVanessaMUellerNo ratings yet
- Diseases With Dermatologic ManifestationsDocument1 pageDiseases With Dermatologic ManifestationsVanessaMUellerNo ratings yet
- Newborn Assessment NORMALDocument2 pagesNewborn Assessment NORMALVanessaMUellerNo ratings yet
- Admission Database PDFDocument6 pagesAdmission Database PDFVanessaMUellerNo ratings yet
- Fluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitDocument1 pageFluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitVanessaMUellerNo ratings yet
- AssessingWounds ProcedureDocument3 pagesAssessingWounds ProcedureVanessaMUellerNo ratings yet
- Nurse Brain Sheet Half SizeDocument1 pageNurse Brain Sheet Half Sizevsosa624No ratings yet
- ManagmentDocument1 pageManagmentVanessaMUellerNo ratings yet
- Alcohol Withdrawal Care PlanDocument1 pageAlcohol Withdrawal Care PlanVanessaMUeller100% (1)
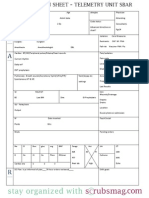
- Nurse Brain Sheet Telemetry Unit SBARDocument1 pageNurse Brain Sheet Telemetry Unit SBARvsosa624No ratings yet
- Nurse Brain Sheet With Shift HoursDocument2 pagesNurse Brain Sheet With Shift HoursLauren Cournoyer Foreman100% (4)
- COPD Care PLAN PDFDocument2 pagesCOPD Care PLAN PDFVanessaMUeller100% (1)
- IV PushDocument3 pagesIV PushVanessaMUeller100% (1)
- Comprehensive Head To Toe Assessment PDFDocument22 pagesComprehensive Head To Toe Assessment PDFVanessaMUellerNo ratings yet
- Example 1 - Focus: Nausea Related To AnestheticDocument1 pageExample 1 - Focus: Nausea Related To AnestheticVanessaMUellerNo ratings yet
- (Chapter 3) : Cell BiologyDocument80 pages(Chapter 3) : Cell BiologyVanessaMUellerNo ratings yet
- AdmimDocument2 pagesAdmimVanessaMUellerNo ratings yet
- Clinical AssessementDocument2 pagesClinical AssessementVanessaMUellerNo ratings yet
- Medication Guide with Side Effects and UsesDocument10 pagesMedication Guide with Side Effects and UsesVanessaMUellerNo ratings yet
- Wound Care PDFDocument100 pagesWound Care PDFVanessaMUeller100% (2)
- HR Ocampo Danilo s2 E10 PDFDocument4 pagesHR Ocampo Danilo s2 E10 PDFVanessaMUellerNo ratings yet
- Nurse Brain Sheet Half SizeDocument1 pageNurse Brain Sheet Half SizeRobyn GrogitskyNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- P T of Comm NSGDocument27 pagesP T of Comm NSGBabita DhruwNo ratings yet
- 26 Sri Rahayu OktavianiDocument123 pages26 Sri Rahayu OktavianiFebrianti FebriantiNo ratings yet
- Pediatric Dentistry Consent For Dental ProceduresDocument2 pagesPediatric Dentistry Consent For Dental ProceduresNishtha KumarNo ratings yet
- Guidelines For Preventing HealthcareDocument78 pagesGuidelines For Preventing HealthcareppeterarmstrongNo ratings yet
- 01 Introduction To Phlebotomy - Wimba DinutanayoDocument14 pages01 Introduction To Phlebotomy - Wimba Dinutanayojamalagus239No ratings yet
- Understanding the pros and cons of early marriage for teenagersDocument15 pagesUnderstanding the pros and cons of early marriage for teenagersShoba ManoharanNo ratings yet
- Human BecomingDocument3 pagesHuman BecomingCharles DaveNo ratings yet
- Rheumatoid Arthritis: Know Your OptionsDocument11 pagesRheumatoid Arthritis: Know Your OptionsMartin UllielNo ratings yet
- Reimplantation of Avulsed Tooth - A Case StudyDocument3 pagesReimplantation of Avulsed Tooth - A Case Studyrahul sharmaNo ratings yet
- Shy BookletDocument28 pagesShy BookletDesmond ScottNo ratings yet
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDateDocument41 pagesStevens-Johnson Syndrome and Toxic Epidermal Necrolysis - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDateDicky SangadjiNo ratings yet
- Bronchitis, Pneumonia and Bronchial Asthma in ChildrenDocument82 pagesBronchitis, Pneumonia and Bronchial Asthma in Childrenstrawberry pieNo ratings yet
- 842 2027 1 SM PDFDocument11 pages842 2027 1 SM PDFAngel Franda PutriNo ratings yet
- Table 2: Endocrine Disorders Disorders Symptoms Lab Test ResultsDocument3 pagesTable 2: Endocrine Disorders Disorders Symptoms Lab Test ResultsRamil BondadNo ratings yet
- An Overview of Asthma Management - UpToDateDocument31 pagesAn Overview of Asthma Management - UpToDateSantiago Mondragon RiosNo ratings yet
- Department of General Surgery: Thermal Injuries Skin Grafts Acute AbdomenDocument115 pagesDepartment of General Surgery: Thermal Injuries Skin Grafts Acute AbdomenAj Christian Lacuesta IsipNo ratings yet
- JSSCPT Physiotherapy HandbookDocument59 pagesJSSCPT Physiotherapy HandbookAbhishek N100% (2)
- Posterior Stabilization of Wedge Compression Fractures with Pedicle Screw FixationDocument7 pagesPosterior Stabilization of Wedge Compression Fractures with Pedicle Screw FixationAlla Yeswanth Dilip KumarNo ratings yet
- Training of Medical Personnel CBRN Nato StandardDocument40 pagesTraining of Medical Personnel CBRN Nato StandardAn Bo0% (1)
- Nitric Acid 70%Document10 pagesNitric Acid 70%Oscar ValdezNo ratings yet
- Respiratory AcidosisDocument6 pagesRespiratory AcidosisSulove KoiralaNo ratings yet
- Journal FoodDocument4 pagesJournal FoodMizaZainalNo ratings yet
- Eucalyptus OilDocument17 pagesEucalyptus OilSorinGeorgeNo ratings yet
- PDPHDocument19 pagesPDPHcardiacanesthesiaNo ratings yet
- Emedicine Hypersemesis GravidarumDocument26 pagesEmedicine Hypersemesis GravidarumAnonymous 3OoumAUytNo ratings yet
- Rayne Yu 16-323 Workout Fitness Training Program AssignmentDocument2 pagesRayne Yu 16-323 Workout Fitness Training Program AssignmentRayne Andreana YuNo ratings yet
- PATHFit I Chapter 4Document6 pagesPATHFit I Chapter 4bamboogabrieltaclaNo ratings yet
- Ovitrelle Epar Medicine Overview - enDocument3 pagesOvitrelle Epar Medicine Overview - enPhysics with V SagarNo ratings yet
- Establishing Positive Family Relationships for Health PromotionDocument78 pagesEstablishing Positive Family Relationships for Health PromotionsunielgowdaNo ratings yet
- 4th Yr SingiDocument322 pages4th Yr SingiSthuti Shetwal100% (1)