You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- PAU Practice Examination (Murcia)Document2 pagesPAU Practice Examination (Murcia)Encarna BMéndezNo ratings yet
- Eye DisordersDocument4 pagesEye DisordersJade SamonteNo ratings yet
- The Benefits of Supplementary Health Insurance Program of "Meuhedet Adif"Document16 pagesThe Benefits of Supplementary Health Insurance Program of "Meuhedet Adif"EnglishAccessibilityNo ratings yet
- PsychiatryDocument5 pagesPsychiatryElyenNo ratings yet
- Pulmocare Datasheet For WebsiteDocument1 pagePulmocare Datasheet For WebsiteOanamikaela VaidaNo ratings yet
- Acid& Chemical Burns Part ADocument10 pagesAcid& Chemical Burns Part ASojiNo ratings yet
- 10.28.21 Ref. 6.08 CCSD MOA CCEA (B)Document7 pages10.28.21 Ref. 6.08 CCSD MOA CCEA (B)FOX5 VegasNo ratings yet
- Ulcerative ColitisDocument9 pagesUlcerative ColitisBheru LalNo ratings yet
- Course: B.Pharm Class: 3 Year Subject: Medicinal Chemistry-I Chapter-1: Basic Principles of Medicinal ChemistryDocument9 pagesCourse: B.Pharm Class: 3 Year Subject: Medicinal Chemistry-I Chapter-1: Basic Principles of Medicinal ChemistryAnanda VijayasarathyNo ratings yet
- Vertigo BPPVDocument2 pagesVertigo BPPVleonjunchan_66965707No ratings yet
- Oppositional Defiant Disorder HandoutDocument3 pagesOppositional Defiant Disorder HandoutKarenJarataNo ratings yet
- Strengthen Your Emotional Agility: A 4-Step Process For Getting UnhookedDocument6 pagesStrengthen Your Emotional Agility: A 4-Step Process For Getting Unhookedneo matrixNo ratings yet
- Case Report VertigoDocument32 pagesCase Report VertigoSuci WulandariNo ratings yet
- Child Health Program Oral Health: Guidance DocumentDocument30 pagesChild Health Program Oral Health: Guidance Documentanubhutigupta1404No ratings yet
- Psychiatric 12Document33 pagesPsychiatric 12Res TyNo ratings yet
- The Lidcombe ProgramDocument12 pagesThe Lidcombe ProgramDemosten100% (1)
- Travel MedicineDocument31 pagesTravel Medicineanshari dwi nugrahaNo ratings yet
- 10-22-14 EditionDocument32 pages10-22-14 EditionSan Mateo Daily JournalNo ratings yet
- Socratic Dialogue and Guided Discovery in Cognitive Behavioral Therapy: A Modified Delphi PanelDocument18 pagesSocratic Dialogue and Guided Discovery in Cognitive Behavioral Therapy: A Modified Delphi PanelMakanudo.No ratings yet
- match01.TWELVE STEP FACILITATION THERAPY MANUAL PDFDocument140 pagesmatch01.TWELVE STEP FACILITATION THERAPY MANUAL PDFsalalepe100% (4)
- Best of Myron NLP UsenetDocument5 pagesBest of Myron NLP Usenetscribd94No ratings yet
- Heart AttackDocument12 pagesHeart AttackPaul NeedhamNo ratings yet
- Inservice PresentationDocument13 pagesInservice Presentationapi-467829418No ratings yet
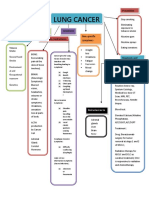
- Concept Map LungDocument1 pageConcept Map LungThea Eya FayeNo ratings yet
- Fatality Inquiry Report: Jeffrey & Jeremy BostickDocument54 pagesFatality Inquiry Report: Jeffrey & Jeremy BostickEmily MertzNo ratings yet
- Ateneo de Zamboanga University: College of Nursing Nursing Skills Output (Nso) Week Biopsy I. DescritptionDocument4 pagesAteneo de Zamboanga University: College of Nursing Nursing Skills Output (Nso) Week Biopsy I. DescritptionHaifi HunNo ratings yet
- Career Interest Profiler ReflectionDocument2 pagesCareer Interest Profiler Reflectionapi-478464529No ratings yet
- 15 Reasons Why Clinical Psychology May Be For YouDocument2 pages15 Reasons Why Clinical Psychology May Be For YouRob SchliffNo ratings yet
- InTech-Management of Bone Loss in Primary and Revision Knee Replacement SurgeryDocument25 pagesInTech-Management of Bone Loss in Primary and Revision Knee Replacement SurgerySagaram ShashidarNo ratings yet
- Rogo Se Bachav, Mohan GuptaDocument122 pagesRogo Se Bachav, Mohan Guptaankurgoel30100% (1)