You might also like
- Modified Bluegrass Appliance PDFDocument4 pagesModified Bluegrass Appliance PDFRenieKumalaNo ratings yet
- Space RegainerDocument7 pagesSpace RegainerdelfNo ratings yet
- Guided Tissue RegenerationDocument4 pagesGuided Tissue RegenerationNicoleta MarcuNo ratings yet
- 1 FrameDentureDocument8 pages1 FrameDentureJennieNo ratings yet
- Classification System For Full EdentulismDocument4 pagesClassification System For Full EdentulismmandakinimohanNo ratings yet
- Review Correlation Between Diabetes Mellitus and Residual Ridge Resorption PDFDocument3 pagesReview Correlation Between Diabetes Mellitus and Residual Ridge Resorption PDFInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Periodontics: Treatment Planning For Patients With Periodontal DiseasesDocument17 pagesPeriodontics: Treatment Planning For Patients With Periodontal Diseasesفاطمة فالح ضايف مزعلNo ratings yet
- Smoking Habits and Alcohol Consumption in Patients Diagnosed With Oral Lichen Planus: A Case ReportDocument17 pagesSmoking Habits and Alcohol Consumption in Patients Diagnosed With Oral Lichen Planus: A Case ReportkuntumNo ratings yet
- Jurnal Reading Bedah MulutDocument27 pagesJurnal Reading Bedah MulutArismunandar SosiloNo ratings yet
- Comparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudyDocument132 pagesComparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudySkAliHassanNo ratings yet
- Provisional Splinting 2013Document87 pagesProvisional Splinting 2013felicedaNo ratings yet
- 1.1 Endodontik: HealingDocument52 pages1.1 Endodontik: HealingARINA KHAQ100% (1)
- Coronoplasty 2Document4 pagesCoronoplasty 2Befalia Aisarahmadani100% (1)
- Clinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFDocument6 pagesClinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFZita AprilliaNo ratings yet
- Arch BarDocument28 pagesArch BarFachrul Latif DentistNo ratings yet
- Space Maintainers: A Review: International Journal of Medical and Health ResearchDocument4 pagesSpace Maintainers: A Review: International Journal of Medical and Health Researchpaper kitaNo ratings yet
- Curve of SpeeDocument7 pagesCurve of SpeeKorina CallerosNo ratings yet
- Comparison of Two Treatment Modalities Operculectomy Vs Thirdmolar Removal For Management of PericoronitisDocument4 pagesComparison of Two Treatment Modalities Operculectomy Vs Thirdmolar Removal For Management of PericoronitisghinaNo ratings yet
- Space Regainers in Pediatric DentistryDocument6 pagesSpace Regainers in Pediatric DentistryFayiz SäbNo ratings yet
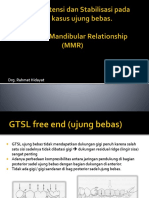
- Dok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRDocument53 pagesDok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRAditya ZulfikarNo ratings yet
- Epulis FissuratumDocument9 pagesEpulis FissuratumDilaC.FareshaNo ratings yet
- SSCDocument10 pagesSSCYanuar MegaNo ratings yet
- Advantages of Balanced Force Technique: Crown-Down (Pressure-Less) TechniqueDocument3 pagesAdvantages of Balanced Force Technique: Crown-Down (Pressure-Less) TechniquejadeNo ratings yet
- Developmental DefectsDocument29 pagesDevelopmental DefectsPrince AhmedNo ratings yet
- IckDocument6 pagesIckbkprosthoNo ratings yet
- Section - 026 - Immediate DenturesDocument12 pagesSection - 026 - Immediate DenturesMuli Maroshi100% (1)
- Systematic Review of Selective GrindingDocument6 pagesSystematic Review of Selective GrindingNiranjanaNo ratings yet
- Ty Removable Orthodontic Appliance For Extrusion ofDocument3 pagesTy Removable Orthodontic Appliance For Extrusion oftyaNo ratings yet
- Kesalahan Radiograf EkstraoralDocument8 pagesKesalahan Radiograf EkstraoralMartyn SuprayugoNo ratings yet
- Majalah IKORTI Desember 2015 PDFDocument56 pagesMajalah IKORTI Desember 2015 PDFAbdi utomoNo ratings yet
- Restorative Technique Selection in Class IV Direct Composite Restorations: A Simplified MethodDocument6 pagesRestorative Technique Selection in Class IV Direct Composite Restorations: A Simplified MethodCalisto GomesNo ratings yet
- Classification of Cleft Lip or PalateDocument15 pagesClassification of Cleft Lip or PalatecempapiNo ratings yet
- Dense Bone Island: Temuan Insidental Pada Radiograf PanoramikDocument4 pagesDense Bone Island: Temuan Insidental Pada Radiograf PanoramikFransiski HoNo ratings yet
- Pre-Prosthetic Treatment and Tooth PreparationDocument45 pagesPre-Prosthetic Treatment and Tooth PreparationJody JodzNo ratings yet
- Bedah Buku Prosto FixDocument22 pagesBedah Buku Prosto FixLeliNo ratings yet
- A Modified Bluegrass Appliance For Interception of Tongue Thrust Habit - A Clinical InnovatiDocument3 pagesA Modified Bluegrass Appliance For Interception of Tongue Thrust Habit - A Clinical InnovatiAdvanced Research PublicationsNo ratings yet
- Jurnal Mounting Articulator PDFDocument6 pagesJurnal Mounting Articulator PDFKhaleda ShafiraNo ratings yet
- Hemiseksi Akar Distal Molar Kedua Rahang BawahDocument5 pagesHemiseksi Akar Distal Molar Kedua Rahang BawahAhmad Willy AntonNo ratings yet
- BionatorDocument10 pagesBionatorDiana DennisNo ratings yet
- Bulk Fill Resin RestorationDocument18 pagesBulk Fill Resin RestorationNuningK93No ratings yet
- Abses IntraoralDocument19 pagesAbses IntraoralTitis LaraswatiNo ratings yet
- Pengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG Denpasar PDFDocument11 pagesPengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG Denpasar PDFZaenuriNo ratings yet
- Prosthodontic DiagnosisDocument15 pagesProsthodontic DiagnosisYashpreetsingh Bhatia100% (1)
- Kanker MulutDocument2 pagesKanker MulutHamba AllahNo ratings yet
- Brochure-Gc Fuji ViiDocument16 pagesBrochure-Gc Fuji ViiZulfahmi NurdinNo ratings yet
- Case Report Fissure SealantDocument8 pagesCase Report Fissure SealantrespikNo ratings yet
- Alternate Technique For Fabrication of A Custom Impression Tray For Definitive Obturator ConstructionDocument3 pagesAlternate Technique For Fabrication of A Custom Impression Tray For Definitive Obturator ConstructionRaven Roth100% (1)
- TUTORIAL IN ENGLISH Blok 12Document7 pagesTUTORIAL IN ENGLISH Blok 12Ifata RDNo ratings yet
- Definitions: - : I) Soft PalateDocument30 pagesDefinitions: - : I) Soft PalateNikita AggarwalNo ratings yet
- Selective GrindingDocument4 pagesSelective GrindingDentist HereNo ratings yet
- Trauma From OcclusionDocument3 pagesTrauma From OcclusionSuganya MurugaiahNo ratings yet
- Oral Wound Healing: Cell Biology and Clinical ManagementFrom EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaNo ratings yet
- Cleft Lip and Palate Management: A Comprehensive AtlasFrom EverandCleft Lip and Palate Management: A Comprehensive AtlasRicardo D. BennunNo ratings yet
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Effects of Orthodontic Treatment With Fixed Appliances On Oral Health Status: A Comprehensive StudyDocument4 pagesEffects of Orthodontic Treatment With Fixed Appliances On Oral Health Status: A Comprehensive StudyPutu WidiastriNo ratings yet
- Bahan Cetak Elastomer PDFDocument4 pagesBahan Cetak Elastomer PDFAstri Ggamjong Xiao LuNo ratings yet
- Clinical Examination of The Temporomandibular JointDocument6 pagesClinical Examination of The Temporomandibular JointAstri Ggamjong Xiao LuNo ratings yet
- Art:10.1186/s40510 016 0154 9 PDFDocument6 pagesArt:10.1186/s40510 016 0154 9 PDFPutu WidiastriNo ratings yet
- Idiopathic Antral Exostoses: Two Rare Cases in Maxillary SinusDocument4 pagesIdiopathic Antral Exostoses: Two Rare Cases in Maxillary SinusAstri Ggamjong Xiao LuNo ratings yet
- Effects of Orthodontic Treatment With Fixed Appliances On Oral Health Status: A Comprehensive StudyDocument4 pagesEffects of Orthodontic Treatment With Fixed Appliances On Oral Health Status: A Comprehensive StudyPutu WidiastriNo ratings yet
- 3g.gingival Retraction TechniquesDocument9 pages3g.gingival Retraction Techniquesdeepakmahla6248No ratings yet
- ADocument5 pagesAAstri Ggamjong Xiao LuNo ratings yet
- VITA 1511GB A Guide To Complete Denture Prosthetics PS EN V00 PDFDocument150 pagesVITA 1511GB A Guide To Complete Denture Prosthetics PS EN V00 PDFAstri Ggamjong Xiao Lu0% (1)
- BDJ 2013. Oral Surgery - Part 3. Temporomandibular DisordersDocument7 pagesBDJ 2013. Oral Surgery - Part 3. Temporomandibular DisordersAstri Ggamjong Xiao LuNo ratings yet
- Removing FPDDocument7 pagesRemoving FPDAntony SebastianNo ratings yet
- Crown and Bridge RemoversDocument8 pagesCrown and Bridge RemoversAstri Ggamjong Xiao LuNo ratings yet
- VITA 1511 VITA 1511E Prothetikleitfaden BA en V01 Screen enDocument150 pagesVITA 1511 VITA 1511E Prothetikleitfaden BA en V01 Screen enAstri Ggamjong Xiao LuNo ratings yet
- Removing Bridge PDFDocument6 pagesRemoving Bridge PDFElbanus WatriNo ratings yet
- DapusDocument1 pageDapusAstri Ggamjong Xiao LuNo ratings yet
- 2014 Article 499Document10 pages2014 Article 499Astri Ggamjong Xiao LuNo ratings yet
- 1472 6831 14 74Document8 pages1472 6831 14 74Astri Ggamjong Xiao LuNo ratings yet
- Module 16 Sawitri-Clinical-Trial 2015Document29 pagesModule 16 Sawitri-Clinical-Trial 2015Astri Ggamjong Xiao LuNo ratings yet
- Base of Tongue VaricesDocument2 pagesBase of Tongue VaricesAstri Ggamjong Xiao LuNo ratings yet
- Clinical Effectiveness and Cost-Effectiveness of Fissure Sealants in Children and Adolescents With A High Caries RiskDocument9 pagesClinical Effectiveness and Cost-Effectiveness of Fissure Sealants in Children and Adolescents With A High Caries RiskAstri Ggamjong Xiao LuNo ratings yet
- Jawetz, Melnick, and Adelberg. (2007) Medical Microbiology 24 Edition. MC Graw HillDocument1 pageJawetz, Melnick, and Adelberg. (2007) Medical Microbiology 24 Edition. MC Graw HillAstri Ggamjong Xiao LuNo ratings yet
- Chronic Inflammation HealingDocument11 pagesChronic Inflammation HealingmemeyviaNo ratings yet
- Targeting Cancer Cells Using PLGA Nanoparticles Surface Modified With Monoclonal AntibodyDocument17 pagesTargeting Cancer Cells Using PLGA Nanoparticles Surface Modified With Monoclonal AntibodyAstri Ggamjong Xiao LuNo ratings yet
- Outer Membrane Protein A From Klebsiella Pneumoniae Activates Bronchial Epithelial Cells Implication in Neutrophil RecruitmentDocument21 pagesOuter Membrane Protein A From Klebsiella Pneumoniae Activates Bronchial Epithelial Cells Implication in Neutrophil RecruitmentAstri Ggamjong Xiao LuNo ratings yet
- 6 Histologi 1 - Jaringan DasarDocument25 pages6 Histologi 1 - Jaringan DasarAstri Ggamjong Xiao LuNo ratings yet
- Synthesis of PLGA Nanoparticles of Tea Polyphenols and Their Strong in Vivo Protective Effect Against Chemically Induced DNA DamageDocument29 pagesSynthesis of PLGA Nanoparticles of Tea Polyphenols and Their Strong in Vivo Protective Effect Against Chemically Induced DNA DamageAstri Ggamjong Xiao LuNo ratings yet
- The Recombinant Klebsiella Pneumoniae Outer Membrane Protein Has Carriers Properties For Conjugated Antigenic PeptideDocument18 pagesThe Recombinant Klebsiella Pneumoniae Outer Membrane Protein Has Carriers Properties For Conjugated Antigenic PeptideAstri Ggamjong Xiao LuNo ratings yet
- Study of The Antibacterial Activities of Soursop (Annona Muricata L.) LeavesDocument8 pagesStudy of The Antibacterial Activities of Soursop (Annona Muricata L.) LeavesAstri Ggamjong Xiao LuNo ratings yet
- Lesson I. Background InformationDocument21 pagesLesson I. Background InformationsuidivoNo ratings yet
- Introduction To The Field of Organizational BehaviorDocument22 pagesIntroduction To The Field of Organizational BehaviorSayyid Al ArizieNo ratings yet
- Sample Internship PPTDocument19 pagesSample Internship PPTSangeeta JamadarNo ratings yet
- Determining Rounding Common CoreDocument2 pagesDetermining Rounding Common Coreapi-3662903730% (1)
- A Tool For The Assessment of Project Com PDFDocument9 pagesA Tool For The Assessment of Project Com PDFgskodikara2000No ratings yet
- Endocrine System Unit ExamDocument3 pagesEndocrine System Unit ExamCHRISTINE JULIANENo ratings yet
- Strategi Pencegahan Kecelakaan Di PT VALE Indonesia Presentation To FPP Workshop - APKPI - 12102019Document35 pagesStrategi Pencegahan Kecelakaan Di PT VALE Indonesia Presentation To FPP Workshop - APKPI - 12102019Eko Maulia MahardikaNo ratings yet
- Customer Refund: Responsibility: Yodlee US AR Super User Navigation: Transactions TransactionsDocument12 pagesCustomer Refund: Responsibility: Yodlee US AR Super User Navigation: Transactions TransactionsAziz KhanNo ratings yet
- The Role of Financial System in DevelopmentDocument5 pagesThe Role of Financial System in DevelopmentCritical ThinkerNo ratings yet
- COMM 103 Floyd Chapters Study GuideDocument4 pagesCOMM 103 Floyd Chapters Study GuideMad BasblaNo ratings yet
- BIO210 Lab Report 3Document6 pagesBIO210 Lab Report 3Isra MallaNo ratings yet
- Tugas, MO - REVIEW JURNAL JIT - Ikomang Aditya Prawira Nugraha (1902612010304)Document12 pagesTugas, MO - REVIEW JURNAL JIT - Ikomang Aditya Prawira Nugraha (1902612010304)MamanxNo ratings yet
- CV AmosDocument4 pagesCV Amoscharity busoloNo ratings yet
- Role of Courts in Granting Bails and Bail Reforms: TH THDocument1 pageRole of Courts in Granting Bails and Bail Reforms: TH THSamarth VikramNo ratings yet
- Oracle QuestDocument521 pagesOracle Questprasanna ghareNo ratings yet
- Filipino HousesDocument4 pagesFilipino HousesjackNo ratings yet
- WHO CDS HIV 19.8 EngDocument24 pagesWHO CDS HIV 19.8 EngMaykel MontesNo ratings yet
- Sickle Cell AnemiaDocument13 pagesSickle Cell Anemiamayra100% (1)
- Full Download Social Animal 14th Edition Aronson Test BankDocument35 pagesFull Download Social Animal 14th Edition Aronson Test Banknaeensiyev100% (32)
- English Lesson PlanDocument3 pagesEnglish Lesson PlanJeremias MartirezNo ratings yet
- A100K10873 VSP-12-Way Technical ManualDocument20 pagesA100K10873 VSP-12-Way Technical Manualchufta50% (2)
- I Wonder Lonely As A Cloud by W. Words WorthDocument6 pagesI Wonder Lonely As A Cloud by W. Words WorthGreen Bergen100% (1)
- Summarized ACLS ScriptDocument7 pagesSummarized ACLS Scriptnc.angel.niceNo ratings yet
- Different Departments Required in A HospitalDocument11 pagesDifferent Departments Required in A HospitalEdsel Dudes AbanteNo ratings yet
- Bubble ColumnDocument34 pagesBubble ColumnihsanNo ratings yet
- Moon and SaturnDocument4 pagesMoon and SaturnRamanasarmaNo ratings yet
- Stroke Practice GuidelineDocument274 pagesStroke Practice GuidelineCamila HernandezNo ratings yet
- Ministry of Truth Big Brother Watch 290123Document106 pagesMinistry of Truth Big Brother Watch 290123Valentin ChirilaNo ratings yet
- OrthoDocument22 pagesOrthosivaleela gNo ratings yet