You might also like
- Cutaneous Sarcoidosis Masquerading AsDocument4 pagesCutaneous Sarcoidosis Masquerading AsIga Nurwani RidwanNo ratings yet
- Esophagitis Dissecans Superficialis With Concomitant BullousDocument4 pagesEsophagitis Dissecans Superficialis With Concomitant BullousIga Nurwani RidwanNo ratings yet
- Pyoderma Gangrenosum A Review of Orthopedic Case ReportsDocument4 pagesPyoderma Gangrenosum A Review of Orthopedic Case ReportsIga Nurwani RidwanNo ratings yet
- Patch Testing in Iranian Children With PDFDocument6 pagesPatch Testing in Iranian Children With PDFIga Nurwani RidwanNo ratings yet
- A Case of Erythrodermia From ExacerbatedDocument4 pagesA Case of Erythrodermia From ExacerbatedIga Nurwani RidwanNo ratings yet
- Yuli Wahyuningsi Linda Lestari Aisyah M.H Ifah Nuryani Miftahul Hilmi Fitriani Tunisah M.Rizalul HaqDocument5 pagesYuli Wahyuningsi Linda Lestari Aisyah M.H Ifah Nuryani Miftahul Hilmi Fitriani Tunisah M.Rizalul HaqIga Nurwani RidwanNo ratings yet
- Pyoderma Gangrenosum: Etiology and PathogenesisDocument13 pagesPyoderma Gangrenosum: Etiology and PathogenesisIga Nurwani RidwanNo ratings yet
- Kanjtan JurnalDocument1 pageKanjtan JurnalIga Nurwani RidwanNo ratings yet
- ContentsDocument2 pagesContentsIga Nurwani RidwanNo ratings yet
- Nego SamplexDocument1 pageNego SamplexZyra C.No ratings yet
- LEaflet SampahDocument3 pagesLEaflet SampahIga Nurwani RidwanNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- UNIT - 3 - GSM Logical Channels and Frame Structure PDFDocument17 pagesUNIT - 3 - GSM Logical Channels and Frame Structure PDFsumanaacharNo ratings yet
- Mas Kaunti, Mas Marami, MagkasingdamiDocument8 pagesMas Kaunti, Mas Marami, MagkasingdamiSherlyn ColobongNo ratings yet
- Neltec Color MG CDocument34 pagesNeltec Color MG CJavier Manuel IbanezNo ratings yet
- Impact of Next-Gen Technologies On Marketing: Manpreet SinghDocument23 pagesImpact of Next-Gen Technologies On Marketing: Manpreet SinghRoronoa ZoldyckNo ratings yet
- Experiment No.1: Design All Gates Using VHDLDocument38 pagesExperiment No.1: Design All Gates Using VHDLashutoshdabas17No ratings yet
- MCS-012 Block 2Document102 pagesMCS-012 Block 2Abhishek VeerkarNo ratings yet
- Factors That Affected Apple Stock PriceDocument8 pagesFactors That Affected Apple Stock PriceSuk Yee Suk YeeNo ratings yet
- Log FarcryDocument7 pagesLog FarcrySergioNo ratings yet
- FS Hotel Jeddah Corniche - Background Music SystemsDocument37 pagesFS Hotel Jeddah Corniche - Background Music SystemsMahmoud MaghrpyNo ratings yet
- MyLabOne - Sat - Touch Service Manual 81B40SM04Document73 pagesMyLabOne - Sat - Touch Service Manual 81B40SM04Sergio Alejandro Castro100% (1)
- Rev.8 RBMviewDocument216 pagesRev.8 RBMviewdford8583No ratings yet
- Electromagnetic Compatibility: Unit-1: Introduction To EmcDocument28 pagesElectromagnetic Compatibility: Unit-1: Introduction To EmcShiva Prasad M100% (1)
- ReadmasterdataDocument3 pagesReadmasterdatagilles777No ratings yet
- 15 - 20 - Manual Pit & Pdit YakogawaDocument61 pages15 - 20 - Manual Pit & Pdit YakogawaWilmar Ortiz MoraNo ratings yet
- AWS Simple-Icons v2.0Document10 pagesAWS Simple-Icons v2.0jonbaerNo ratings yet
- CodetantraDocument51 pagesCodetantrapratik ghoshNo ratings yet
- B DP Mail Exc Guide WinDocument254 pagesB DP Mail Exc Guide WinvamsiNo ratings yet
- Ecf2 Module 2Document6 pagesEcf2 Module 2Blackwolf SocietyNo ratings yet
- Automatic Period OpeningDocument21 pagesAutomatic Period Openingcdhars100% (1)
- Energy: Akshay Ajagekar, Fengqi YouDocument14 pagesEnergy: Akshay Ajagekar, Fengqi YouDANTENo ratings yet
- Introduction To Computing Fundamentals of ICT Week 1-2Document21 pagesIntroduction To Computing Fundamentals of ICT Week 1-2Ronald Cambil Jr.No ratings yet
- 8-Port Arbiter Specifications for Fixed Priority and Round Robin SchemesDocument4 pages8-Port Arbiter Specifications for Fixed Priority and Round Robin SchemesAnonymous ptSFzcfNo ratings yet
- Asian Air Lines VisionDocument13 pagesAsian Air Lines VisionMusaab QamarNo ratings yet
- Inventory Management System UML Diagram - CompleteDocument15 pagesInventory Management System UML Diagram - CompleteHuda Al-Shuhayeb100% (1)
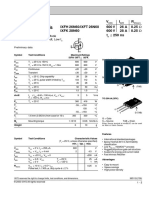
- Hiperfet Power Mosfets: V I R Ixfh 26N60/Ixft 26N60 600 V 26 A 0.25 Ixfk 28N60 600 V 28 A 0.25 T 250 NsDocument2 pagesHiperfet Power Mosfets: V I R Ixfh 26N60/Ixft 26N60 600 V 26 A 0.25 Ixfk 28N60 600 V 28 A 0.25 T 250 NsAmirNo ratings yet
- Physics RefractionDocument15 pagesPhysics RefractionFelicity O' MalleyNo ratings yet
- English Turkish 2008-11-15Document30 pagesEnglish Turkish 2008-11-15RoyMarie100% (1)
- Feature Boxes CV TemplateDocument3 pagesFeature Boxes CV TemplatezaidkhanNo ratings yet
- Jiwaji University Gwalior: Self Learning Material FORDocument359 pagesJiwaji University Gwalior: Self Learning Material FORVikas SharmaNo ratings yet
- Features: Dual, Low Power CMOS Operational AmplifiersDocument9 pagesFeatures: Dual, Low Power CMOS Operational AmplifiersDibya DeyNo ratings yet