You might also like
- Human Anatomy QsDocument31 pagesHuman Anatomy QsAzhagar Ramesh SNo ratings yet
- Hamstring Injuries in Football PDFDocument276 pagesHamstring Injuries in Football PDFulfahrifNo ratings yet
- Thesis Protocol Final SarangDocument26 pagesThesis Protocol Final SarangRaj KotichaNo ratings yet
- HerbalismDocument18 pagesHerbalismmieNo ratings yet
- Nursing Management HydrocephalusDocument4 pagesNursing Management HydrocephalusPrecious Mae Benologa100% (1)
- Stages of Labor and DeliveryDocument4 pagesStages of Labor and DeliveryvienreyNo ratings yet
- Retinos PDFDocument83 pagesRetinos PDFPaulo Gan100% (2)
- Emqs ObsDocument33 pagesEmqs Obsbakkiaha100% (1)
- NURSING BOOK LIST - Docx FinalDocument10 pagesNURSING BOOK LIST - Docx FinalChaitanya RkNo ratings yet
- Radiology Procedure ManualDocument29 pagesRadiology Procedure ManualAnonymous ic2CDkF100% (1)
- AutomaticLiverTumor PDFDocument18 pagesAutomaticLiverTumor PDFMuhammad Zaka Ud DinNo ratings yet
- Liver Tumor SegmentationDocument17 pagesLiver Tumor SegmentationtamascristianpetruNo ratings yet
- Recist 1Document11 pagesRecist 1Kelik WagiyantoNo ratings yet
- Utilidad de Los Metodos de Segmentacion HepaticaDocument17 pagesUtilidad de Los Metodos de Segmentacion HepaticaJardeli MerinoNo ratings yet
- Three-Dimensional Conformal Radiation Therapy (3DCRT) For Prostate CancerDocument34 pagesThree-Dimensional Conformal Radiation Therapy (3DCRT) For Prostate CancerMuhammad Safwan Ahmad FadzilNo ratings yet
- ABSTRACTDocument22 pagesABSTRACTPhalguni ShenoyNo ratings yet
- Automated Detection and Segmentation of Large Lesions in CT ColonographyDocument10 pagesAutomated Detection and Segmentation of Large Lesions in CT ColonographyFathullah MuhammadNo ratings yet
- Performance Evaluation of TumorDocument12 pagesPerformance Evaluation of TumorAnonymous lVQ83F8mCNo ratings yet
- The Applications of Radiomics in Precision Diagnosis and Treatment of OncologyDocument42 pagesThe Applications of Radiomics in Precision Diagnosis and Treatment of Oncologyyuta titeNo ratings yet
- A Novel Breast Tumor Classification Using Neutrosophic Score FeaturesDocument11 pagesA Novel Breast Tumor Classification Using Neutrosophic Score FeaturesMia AmaliaNo ratings yet
- Comparison of Retropubic, Laparoscopic and Robotic Radical ProstatectomyDocument13 pagesComparison of Retropubic, Laparoscopic and Robotic Radical ProstatectomyOrlando SotoNo ratings yet
- RPD Group6 Draft v4 04172024-2Document4 pagesRPD Group6 Draft v4 04172024-2api-691667702No ratings yet
- Research ProposalDocument4 pagesResearch Proposalapi-710804215No ratings yet
- Cancers 14 05841 v2Document21 pagesCancers 14 05841 v2someonefromsomwhere123No ratings yet
- Mri Report RectumDocument1 pageMri Report RectumChar CharNo ratings yet
- Hepatocellular Carcinoma Project DescriptionDocument6 pagesHepatocellular Carcinoma Project DescriptionAmandeep NehraNo ratings yet
- 1 - APJCP - Volume 17 - Issue 2 - Pages 823-827Document5 pages1 - APJCP - Volume 17 - Issue 2 - Pages 823-827chaimaa aouicheNo ratings yet
- Adjuvant Therapy in The Treatment of Gallbladder Cancer: A Meta-AnalysisDocument10 pagesAdjuvant Therapy in The Treatment of Gallbladder Cancer: A Meta-Analysisdewi keliNo ratings yet
- Surgery: SciencedirectDocument7 pagesSurgery: SciencedirectAriska Nur FitrianaNo ratings yet
- Lung Cancer Detection Using Image Processing PDFDocument7 pagesLung Cancer Detection Using Image Processing PDFAishwaryaNo ratings yet
- PET in OncologyDocument70 pagesPET in Oncologyg_daniel119974No ratings yet
- Dosimetric Comparison of AcurosBV With AAPMDocument19 pagesDosimetric Comparison of AcurosBV With AAPMBruno MendesNo ratings yet
- Final DraftDocument18 pagesFinal Draftapi-334402872No ratings yet
- 2023 Radiomics Prognostic Analysis of PETCT Images in A Multicenter Head and Neck Cancer CohortDocument15 pages2023 Radiomics Prognostic Analysis of PETCT Images in A Multicenter Head and Neck Cancer CohortT.h. HuangNo ratings yet
- Perioperative Factors Associated With Survival Following Surgery For Pancreatic Cancer - A Nationwide Analysis of 473 Cases From DenmarkDocument11 pagesPerioperative Factors Associated With Survival Following Surgery For Pancreatic Cancer - A Nationwide Analysis of 473 Cases From DenmarkDr Supriya SaxenaNo ratings yet
- Lectura 1Document13 pagesLectura 1Ricardo Huaman QuirozNo ratings yet
- 2022 48 3 3675 EnglishDocument10 pages2022 48 3 3675 EnglishRaul Matute MartinNo ratings yet
- BJC 2013473 ADocument9 pagesBJC 2013473 AAlex SemenzatoNo ratings yet
- Imagerie DG CHCDocument16 pagesImagerie DG CHCnessimNo ratings yet
- Lee. C. D.Document14 pagesLee. C. D.GiovanniNo ratings yet
- Prostate Segmentation ThesisDocument9 pagesProstate Segmentation Thesisgj9ggjry100% (2)
- 1 s2.0 S0960977620302071 MainDocument8 pages1 s2.0 S0960977620302071 MainAchdewa RohmatullahNo ratings yet
- Esofago Cervical Metaanalisis de Virgilio 2022Document13 pagesEsofago Cervical Metaanalisis de Virgilio 2022Carlos N. Rojas PuyolNo ratings yet
- Apendicitis Aguda PDFDocument42 pagesApendicitis Aguda PDFSamariss DuranNo ratings yet
- Bài báo khoa học buổi 1Document10 pagesBài báo khoa học buổi 1Giang Nguyễn ThùyNo ratings yet
- Computers in Biology and Medicine: Vida Harati, Rasoul Khayati, Abdolreza FarzanDocument10 pagesComputers in Biology and Medicine: Vida Harati, Rasoul Khayati, Abdolreza FarzanJosé Ignacio OrlandoNo ratings yet
- PalateDocument41 pagesPalatearif sudiantoNo ratings yet
- Semiautomated Segmentation of Head and Neck Cancers in 18F-FDG PET Scans: A Just-Enough-Interaction ApproachDocument17 pagesSemiautomated Segmentation of Head and Neck Cancers in 18F-FDG PET Scans: A Just-Enough-Interaction ApproachPuig CozarNo ratings yet
- Matsuda 2014Document8 pagesMatsuda 2014Adrian SilaghiNo ratings yet
- 464 2016 Article 4752Document23 pages464 2016 Article 4752maria.fetterNo ratings yet
- Liver Cancer Detection Survey PaperDocument8 pagesLiver Cancer Detection Survey PaperHarshitha HarshuNo ratings yet
- 2023 BMC UrologyDocument18 pages2023 BMC Urologyyicini2524No ratings yet
- 1 s2.0 S1361841520302838 MainDocument11 pages1 s2.0 S1361841520302838 Mainedfewf3No ratings yet
- Automated Segmentation and Classi Fication of Hepatocellular Carcinoma Using Fuzzy C-Means and SVMDocument18 pagesAutomated Segmentation and Classi Fication of Hepatocellular Carcinoma Using Fuzzy C-Means and SVMBudi Utami FahnunNo ratings yet
- Accuracy of Real-Time Shear Wave Elastography in SDocument10 pagesAccuracy of Real-Time Shear Wave Elastography in SApotik ApotekNo ratings yet
- Mortality and Infectious Complications of Therapeutic Endovascular Interventional Radiology: A Systematic and Meta-Analysis ProtocolDocument8 pagesMortality and Infectious Complications of Therapeutic Endovascular Interventional Radiology: A Systematic and Meta-Analysis ProtocolgtNo ratings yet
- Keywords Mammogram Adaptive Median Filter GMM Segmentation HMRF-EM GLCMDocument13 pagesKeywords Mammogram Adaptive Median Filter GMM Segmentation HMRF-EM GLCMChamar AshishNo ratings yet
- Pancreatic Duct TextureDocument9 pagesPancreatic Duct TextureAdarsh GhoshNo ratings yet
- Efficacy of Minimally Invasive Surgery On Giant Cell Tumor of The Bone: A Systematic ReviewDocument14 pagesEfficacy of Minimally Invasive Surgery On Giant Cell Tumor of The Bone: A Systematic ReviewAnonymous MLXWLzNo ratings yet
- 10.1007@s13304 019 00648 XDocument8 pages10.1007@s13304 019 00648 XGabriel RangelNo ratings yet
- 2020 World Society of Emergency Surgery Updated Guidelines For The Diagnosis and Treatment of Acute Calculus CholecystitisDocument26 pages2020 World Society of Emergency Surgery Updated Guidelines For The Diagnosis and Treatment of Acute Calculus CholecystitisDiego Andres VasquezNo ratings yet
- Perfusion 1Document12 pagesPerfusion 1zixdiddyNo ratings yet
- Ejsr 72 3 04Document9 pagesEjsr 72 3 04Khalifa BakkarNo ratings yet
- Current and Future Use of Radiological Images in The Management of Gynecological Malignancies - A Survey of Practice in The UKDocument21 pagesCurrent and Future Use of Radiological Images in The Management of Gynecological Malignancies - A Survey of Practice in The UKKrishna PanduNo ratings yet
- Ovarian Cancer An Update On Imaging in The - 2019 - Diagnostic and InterventioDocument9 pagesOvarian Cancer An Update On Imaging in The - 2019 - Diagnostic and Interventiosica_17_steaua6519No ratings yet
- Exercise and Colorectal Cancer: A Systematic Review and Meta-Analysis of Exercise Safety, Feasibility and EffectivenessDocument14 pagesExercise and Colorectal Cancer: A Systematic Review and Meta-Analysis of Exercise Safety, Feasibility and EffectivenessDidi Nurhadi IllianNo ratings yet
- 2016 Article 826Document6 pages2016 Article 826tomniucNo ratings yet
- Automatic Expert Diagnostic System For CRC Detection: Hiba A. Muhareb, Sara Tedmori, Kais HasanDocument4 pagesAutomatic Expert Diagnostic System For CRC Detection: Hiba A. Muhareb, Sara Tedmori, Kais HasanUbiquitous Computing and Communication JournalNo ratings yet
- Therapy Response Imaging in OncologyFrom EverandTherapy Response Imaging in OncologyMizuki NishinoNo ratings yet
- Neutrosophic Triplet Normed Ring SpaceDocument8 pagesNeutrosophic Triplet Normed Ring SpaceMia AmaliaNo ratings yet
- Single Valued Neutrosophic Numbers and Analytic Hierarchy Process For Project SelectionDocument9 pagesSingle Valued Neutrosophic Numbers and Analytic Hierarchy Process For Project SelectionMia AmaliaNo ratings yet
- On Neutrosophic Crisp Semi Alpha Closed SetsDocument8 pagesOn Neutrosophic Crisp Semi Alpha Closed SetsMia AmaliaNo ratings yet
- Multi-Objective Portfolio Selection Model With Diversification by Neutrosophic Optimization TechniqueDocument10 pagesMulti-Objective Portfolio Selection Model With Diversification by Neutrosophic Optimization TechniqueMia AmaliaNo ratings yet
- Neutrosophic Crisp Bi-Topological SpacesDocument8 pagesNeutrosophic Crisp Bi-Topological SpacesMia AmaliaNo ratings yet
- Neutrosophic Units of Neutrosophic Rings and FieldsDocument8 pagesNeutrosophic Units of Neutrosophic Rings and FieldsMia AmaliaNo ratings yet
- On Geodesics of The Tangent and Normal Surfaces Defined by TN-Smarandache Curve According To Frenet FrameDocument1 pageOn Geodesics of The Tangent and Normal Surfaces Defined by TN-Smarandache Curve According To Frenet FrameMia AmaliaNo ratings yet
- Single-Valued Neutrosophic HypergraphsDocument14 pagesSingle-Valued Neutrosophic HypergraphsMia AmaliaNo ratings yet
- A Revisit To NC-VIKOR Based MAGDM Strategy in Neutrosophic Cubic Set EnvironmentDocument11 pagesA Revisit To NC-VIKOR Based MAGDM Strategy in Neutrosophic Cubic Set EnvironmentMia AmaliaNo ratings yet
- An Inventory Model Under Space Constraint in Neutrosophic Environment: A Neutrosophic Geometric Programming ApproachDocument17 pagesAn Inventory Model Under Space Constraint in Neutrosophic Environment: A Neutrosophic Geometric Programming ApproachMia AmaliaNo ratings yet
- Bi-Level Linear Programming Problem With Neutrosophic NumbersDocument12 pagesBi-Level Linear Programming Problem With Neutrosophic NumbersMia AmaliaNo ratings yet
- On Smarandache Curves of Involute-Evolute Curve According To Frenet Frame in Minkowski 3-SpaceDocument1 pageOn Smarandache Curves of Involute-Evolute Curve According To Frenet Frame in Minkowski 3-SpaceMia AmaliaNo ratings yet
- Smarandache Curves According To Q-Frame in Euclidean 3-SpaceDocument2 pagesSmarandache Curves According To Q-Frame in Euclidean 3-SpaceMia AmaliaNo ratings yet
- Smarandache Curves of Bertrand Curves Pair According To Frenet FrameDocument11 pagesSmarandache Curves of Bertrand Curves Pair According To Frenet FrameMia AmaliaNo ratings yet
- A Generalization of Surfaces Family With Common Smarandache Asymptotic Curves in Galilean SpaceDocument1 pageA Generalization of Surfaces Family With Common Smarandache Asymptotic Curves in Galilean SpaceMia AmaliaNo ratings yet
- A Forecasting Model Based On Multi-Valued Neutrosophic Sets and Two-Factor, Third-Order Fuzzy Fluctuation Logical RelationshipsDocument18 pagesA Forecasting Model Based On Multi-Valued Neutrosophic Sets and Two-Factor, Third-Order Fuzzy Fluctuation Logical RelationshipsMia AmaliaNo ratings yet
- A Neutrosophic Set Based Fault Diagnosis Method Based On Multi-Stage Fault Template DataDocument16 pagesA Neutrosophic Set Based Fault Diagnosis Method Based On Multi-Stage Fault Template DataMia AmaliaNo ratings yet
- Some Generalized Dice Measures For Double-Valued Neutrosophic Sets and Their ApplicationsDocument16 pagesSome Generalized Dice Measures For Double-Valued Neutrosophic Sets and Their ApplicationsMia AmaliaNo ratings yet
- Fixed Point Theorem For Neutrosophic Triplet Partial Metric SpaceDocument7 pagesFixed Point Theorem For Neutrosophic Triplet Partial Metric SpaceMia AmaliaNo ratings yet
- Fundamental Homomorphism Theorems For Neutrosophic Extended Triplet GroupsDocument14 pagesFundamental Homomorphism Theorems For Neutrosophic Extended Triplet GroupsMia AmaliaNo ratings yet
- Research On Construction Engineering Project Risk Assessment With Some 2-Tuple Linguistic Neutrosophic Hamy Mean OperatorsDocument26 pagesResearch On Construction Engineering Project Risk Assessment With Some 2-Tuple Linguistic Neutrosophic Hamy Mean OperatorsMia AmaliaNo ratings yet
- Design of Fuzzy Cognitive Model of Mutual Influence and Connectivity of Innovative TechnologiesDocument7 pagesDesign of Fuzzy Cognitive Model of Mutual Influence and Connectivity of Innovative TechnologiesMia AmaliaNo ratings yet
- Dual Generalized Nonnegative Normal Neutrosophic Bonferroni Mean Operators and Their Application in Multiple Attribute Decision MakingDocument19 pagesDual Generalized Nonnegative Normal Neutrosophic Bonferroni Mean Operators and Their Application in Multiple Attribute Decision MakingMia AmaliaNo ratings yet
- Some Generalized Dice Measures For Double-Valued Neutrosophic Sets and Their ApplicationsDocument18 pagesSome Generalized Dice Measures For Double-Valued Neutrosophic Sets and Their ApplicationsMia AmaliaNo ratings yet
- An OWA Distance-Based, Single-Valued Neutrosophic Linguistic TOPSIS Approach For Green Supplier Evaluation and Selection in Low-Carbon Supply ChainsDocument15 pagesAn OWA Distance-Based, Single-Valued Neutrosophic Linguistic TOPSIS Approach For Green Supplier Evaluation and Selection in Low-Carbon Supply ChainsMia AmaliaNo ratings yet
- Different Methodologies in Treating UncertaintyDocument7 pagesDifferent Methodologies in Treating UncertaintyMia AmaliaNo ratings yet
- The Location Selection For Roundabout Construction Using Rough BWM-Rough WASPAS Approach Based On A New Rough Hamy AggregatorDocument29 pagesThe Location Selection For Roundabout Construction Using Rough BWM-Rough WASPAS Approach Based On A New Rough Hamy AggregatorMia AmaliaNo ratings yet
- 1 15 AstrovirusDocument16 pages1 15 AstrovirusRizal Hery100% (1)
- Are Errors in Otorhinolaryngology Always A Sign of Medical MalpracticeDocument7 pagesAre Errors in Otorhinolaryngology Always A Sign of Medical MalpracticeMyrellaAlexandraNo ratings yet
- Mic Eales A Visual Enquiry Into SuicideDocument4 pagesMic Eales A Visual Enquiry Into Suicidemaribolla8015No ratings yet
- Effectiveness of A Comprehensive Hand Hygiene Program ForDocument11 pagesEffectiveness of A Comprehensive Hand Hygiene Program Form1k0eNo ratings yet
- Endocrine Glands The Producers of Chemical MessengersDocument10 pagesEndocrine Glands The Producers of Chemical Messengersahmed100% (1)
- Cassida Fluid GL 220-SdsDocument5 pagesCassida Fluid GL 220-SdsFajar EkoNo ratings yet
- Duty Report RIWDocument41 pagesDuty Report RIWRiyan W. PratamaNo ratings yet
- Pedia Small Notebook Edited PDFDocument17 pagesPedia Small Notebook Edited PDFAshNo ratings yet
- Gpat 2019Document51 pagesGpat 2019Nishabh KushwahaNo ratings yet
- Intramedullary Nailing For Femur Fracture Web Version EnglishDocument6 pagesIntramedullary Nailing For Femur Fracture Web Version EnglishCarima JatnoNo ratings yet
- Traction PDFDocument31 pagesTraction PDFrushaliNo ratings yet
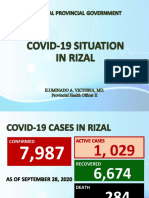
- Covid19 Situation in RizalDocument23 pagesCovid19 Situation in RizalToni Quitalig GamezNo ratings yet
- Aseptic MeningitisDocument24 pagesAseptic Meningitisidno1008100% (1)
- Police Log November 7, 2016Document13 pagesPolice Log November 7, 2016MansfieldMAPoliceNo ratings yet
- Avicenna's Canon of MedicineDocument8 pagesAvicenna's Canon of MedicinelearnafrenNo ratings yet
- Daftar ObatDocument27 pagesDaftar Obathanny nuguNo ratings yet
- Pain ADocument19 pagesPain Akcc2012No ratings yet
- A New Lingual Straight-Wire Techique: Journal of Clinical Orthodontics: JCO February 2010Document11 pagesA New Lingual Straight-Wire Techique: Journal of Clinical Orthodontics: JCO February 2010Hafaifa TaiebNo ratings yet
- Maquet Meera BrochureDocument16 pagesMaquet Meera BrochureFeridun MADRANNo ratings yet
- Skin Care Plan: Nu Derm Protocol ForDocument7 pagesSkin Care Plan: Nu Derm Protocol ForsheilaNo ratings yet
- OrthopedicDocument1 pageOrthopedicapi-352507025No ratings yet