You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Pathophysiology of FractureDocument2 pagesPathophysiology of FractureAnne Lorraine Bringas93% (27)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Nursing Students Peritonitis Care PlanDocument2 pagesNursing Students Peritonitis Care PlanJide Manuel100% (1)
- Reversible and Irreversible Cell InjuryDocument55 pagesReversible and Irreversible Cell Injurygabb bbNo ratings yet
- Pharyngitis. NCPDocument2 pagesPharyngitis. NCPbiancaNo ratings yet
- MSM Information BookletDocument36 pagesMSM Information Bookletzimko100% (3)
- Case Study Neonatal SepsisDocument21 pagesCase Study Neonatal SepsisLenjun0% (1)
- EULAR Points To Consider For The Management of Difficult To Treat Rheumatoid ArthritisDocument14 pagesEULAR Points To Consider For The Management of Difficult To Treat Rheumatoid ArthritisseleneNo ratings yet
- Chapter One The Problem and Its Background 1.1 Introduction of The StudyDocument37 pagesChapter One The Problem and Its Background 1.1 Introduction of The StudyJanelyn GarinNo ratings yet
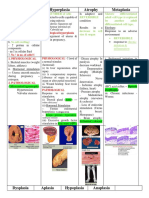
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocument20 pagesHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNo ratings yet
- Patofisiologi GBSDocument9 pagesPatofisiologi GBSIrma SavitriNo ratings yet
- Pneumonia PathophysiologyDocument1 pagePneumonia PathophysiologyDee Sarajan100% (3)
- 2nd Open Book Exam, Aseel AlharbiDocument6 pages2nd Open Book Exam, Aseel Alharbiعبدالرحمن الحربيNo ratings yet
- Allergy Essentials 2Nd Edition Robyn E Ohehir Full ChapterDocument51 pagesAllergy Essentials 2Nd Edition Robyn E Ohehir Full Chapterrobert.collin594100% (8)
- Cell Injury and Cellular AdaptationDocument30 pagesCell Injury and Cellular AdaptationAngelita RuntukNo ratings yet
- Deep Transverse MassageDocument9 pagesDeep Transverse MassageAmimul EhsanNo ratings yet
- Dr. Ranjita Singh Department of PathologyDocument19 pagesDr. Ranjita Singh Department of PathologyMohan Prasad GuptaNo ratings yet
- Emphasis of Yoga in The Management of Diabetes 2155 6156 1000613Document11 pagesEmphasis of Yoga in The Management of Diabetes 2155 6156 1000613AnuradhatagoreNo ratings yet
- GP Factsheet - Steroids and The EyeDocument6 pagesGP Factsheet - Steroids and The EyeBima RizkiNo ratings yet
- Infectious DiseasesDocument6 pagesInfectious DiseasesAlexa QuizomNo ratings yet
- 1-S2.0-S2352939316000026-Main Microbiomul Si Glicemia PDFDocument15 pages1-S2.0-S2352939316000026-Main Microbiomul Si Glicemia PDFLUTICHIEVICI NATALIANo ratings yet
- Personal HygiineDocument6 pagesPersonal HygiineYennyNo ratings yet
- Assessment Diagnosis Planning Implementation Rationale Desired Outcomes Subjective: "Napakasakit NG Mga Kasukasuhan Ko" As Verbalized by The PatientDocument5 pagesAssessment Diagnosis Planning Implementation Rationale Desired Outcomes Subjective: "Napakasakit NG Mga Kasukasuhan Ko" As Verbalized by The PatientAngelou Mortos100% (1)
- Mindfulness Based Stress Reduction: An Integrated View of Physiological and Molecular Aspects of Mindfulness Intervention On Stress ManagementDocument14 pagesMindfulness Based Stress Reduction: An Integrated View of Physiological and Molecular Aspects of Mindfulness Intervention On Stress ManagementajmrdNo ratings yet
- Perez-Cerdá - Inflammation Neurodegeneration Multiple SclerosisDocument8 pagesPerez-Cerdá - Inflammation Neurodegeneration Multiple SclerosisinesNo ratings yet
- Kim1985 PDFDocument7 pagesKim1985 PDFfadwa lachkerNo ratings yet
- Unit - Two - Infection Control - Universal PrecautionsDocument31 pagesUnit - Two - Infection Control - Universal Precautionsvirtus_kuwaitNo ratings yet
- Speciality: General Medicine Case: Nephrotic Syndrome HistoryDocument49 pagesSpeciality: General Medicine Case: Nephrotic Syndrome Historydrtpk100% (2)
- Wrist Pulsating Laser HOEKO - 350 (Semiconductor Device For Laser TherapyDocument30 pagesWrist Pulsating Laser HOEKO - 350 (Semiconductor Device For Laser TherapysumarumNo ratings yet
- Article in Press: SarcopeniaDocument6 pagesArticle in Press: SarcopeniaLucas CardosoNo ratings yet
- KeratitisDocument26 pagesKeratitisHIDAYATUL RAHMINo ratings yet