You might also like
- The Role of Creativity in EntrepreneurshipDocument35 pagesThe Role of Creativity in Entrepreneurshipscorpion999No ratings yet
- Using Mind Power and Affirmations 6 PagesDocument6 pagesUsing Mind Power and Affirmations 6 Pagesscorpion999No ratings yet
- Ralf General Assessment Profile !Document20 pagesRalf General Assessment Profile !scorpion999No ratings yet
- A Complete Program For Living An Uncommon Life 63 PagesDocument4 pagesA Complete Program For Living An Uncommon Life 63 Pagesscorpion999No ratings yet
- Beliefchange 29 Pages PDFDocument29 pagesBeliefchange 29 Pages PDFscorpion999100% (1)
- Table 3: Nutritional Goals For Proposed Daily Food Intake Patterns Page 1, Goals For VitaminsDocument4 pagesTable 3: Nutritional Goals For Proposed Daily Food Intake Patterns Page 1, Goals For Vitaminsscorpion999No ratings yet
- Controlmind 25 PagesDocument25 pagesControlmind 25 Pagesscorpion999No ratings yet
- Gloria Gonzalez: Reborn: The Wanderer in US Hispanic Literature. Sancho Rodriguez, ChairDocument2 pagesGloria Gonzalez: Reborn: The Wanderer in US Hispanic Literature. Sancho Rodriguez, Chairscorpion999No ratings yet
- Assistant Accountant CV TemplateDocument2 pagesAssistant Accountant CV Templatescorpion999No ratings yet
- Rita CVDocument2 pagesRita CVscorpion999No ratings yet
- Zap Your LifeDocument27 pagesZap Your Lifescorpion999No ratings yet
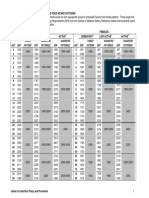
- Target Suggested Suggested Target Suggested Suggested AGE EER Pattern EER Pattern (S) EER Pattern (S) AGE EER Pattern EER Pattern (S) EER Pattern (S)Document2 pagesTarget Suggested Suggested Target Suggested Suggested AGE EER Pattern EER Pattern (S) EER Pattern (S) AGE EER Pattern EER Pattern (S) EER Pattern (S)scorpion999No ratings yet
- Iabc in Numbers: Connect With UsDocument2 pagesIabc in Numbers: Connect With Usscorpion999No ratings yet
- Agenda: TRX Suspension Trainer CourseDocument1 pageAgenda: TRX Suspension Trainer Coursescorpion999No ratings yet
- Rita CVDocument2 pagesRita CVscorpion999No ratings yet
- July - August Training2Document7 pagesJuly - August Training2scorpion999No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Look and Feel Better MenDocument83 pagesLook and Feel Better MenPedro Ortiz Sanchez0% (1)
- King of Weighted 1RM Edition - Michael Schulz PDFDocument36 pagesKing of Weighted 1RM Edition - Michael Schulz PDFLuca Delvecchio100% (4)
- Conjugate Club Olympic Weightlifting Workouts Month 1Document4 pagesConjugate Club Olympic Weightlifting Workouts Month 1vNo ratings yet
- Exercise Duration: Yes NoDocument8 pagesExercise Duration: Yes NodddNo ratings yet
- Project Physique - Beginner ProgramsDocument45 pagesProject Physique - Beginner Programsbomo romoNo ratings yet
- Reform - The 12-Week Transformation Workout Plan - Muscle & FitnessDocument17 pagesReform - The 12-Week Transformation Workout Plan - Muscle & FitnessShivprasad SavadattiNo ratings yet
- GET RIPPED Workout Plan by Guru Mann PDFDocument2 pagesGET RIPPED Workout Plan by Guru Mann PDFkhalidNo ratings yet
- Mass Performance ProgramDocument9 pagesMass Performance ProgramNguyễn DươngNo ratings yet
- Competitor Day 4Document17 pagesCompetitor Day 4Lulu JoisinNo ratings yet
- David Laid DUP ProgramDocument12 pagesDavid Laid DUP Programshiv kakkar50% (24)
- CTFletcherarms v1Document11 pagesCTFletcherarms v1seenyb100% (9)
- Jay ManualDocument17 pagesJay ManualAbraham Hernandez89% (19)
- Best Upper Body Workout RoutineDocument35 pagesBest Upper Body Workout RoutineMATHIEU95120No ratings yet
- Goalkeepers TrainingDocument5 pagesGoalkeepers TrainingMaradona MatiusNo ratings yet
- Powerbridge Prime: Jack MorrowDocument9 pagesPowerbridge Prime: Jack MorrowLuis Zavala100% (1)
- Week 1: DAY 1 - Chest/Shoulders/TricepsDocument5 pagesWeek 1: DAY 1 - Chest/Shoulders/TricepsYashNo ratings yet
- 6 Weeks To Sick Arms by Jim StoppaniDocument6 pages6 Weeks To Sick Arms by Jim Stoppanimohamed aliNo ratings yet
- The Periodization BibleDocument41 pagesThe Periodization BibleKyle Carter100% (1)
- Westside Conjugate CalculatorDocument10 pagesWestside Conjugate Calculatorp300644No ratings yet
- Raph Planned Workout Routine by SixtusDocument4 pagesRaph Planned Workout Routine by Sixtuscliffordtor16No ratings yet
- 5 Day Push Pull Leg SplitDocument4 pages5 Day Push Pull Leg SplitSudeep NNo ratings yet
- Mass Training 12 WeeksDocument3 pagesMass Training 12 WeeksharaNo ratings yet
- Arnold Dumbbell Press: Exercise DataDocument25 pagesArnold Dumbbell Press: Exercise Dataaries_02No ratings yet
- SBD WorkoutDocument25 pagesSBD WorkoutJakob BEnigerNo ratings yet
- Arnold Mass 1Document13 pagesArnold Mass 1Abdul-Raheem MohammedNo ratings yet
- Build Your Own HypertrophyDocument33 pagesBuild Your Own Hypertrophyaeu3csd bdvt100% (1)
- Skill XDocument7 pagesSkill Xdisdemasrl.obra21No ratings yet
- Traps, Delts & NeckDocument2 pagesTraps, Delts & NecknehapanditayinNo ratings yet
- NJBDocument4 pagesNJBTijanaNedićNo ratings yet
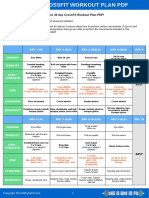
- 30 Day Crossfit Workout PlanDocument3 pages30 Day Crossfit Workout PlanadrienNo ratings yet