You might also like
- MSL 2019 68Document10 pagesMSL 2019 68giviNo ratings yet
- Jadwal QR Bulan AprilDocument12 pagesJadwal QR Bulan AprilgiviNo ratings yet
- Hasil Nilai Pre Post TestDocument1 pageHasil Nilai Pre Post TestgiviNo ratings yet
- Data by Name Lansia Desa TambakDocument41 pagesData by Name Lansia Desa TambakgiviNo ratings yet
- List Pasien Ranap: Tanggal: 24 November 2021 Dokter: GiviDocument18 pagesList Pasien Ranap: Tanggal: 24 November 2021 Dokter: GivigiviNo ratings yet
- Morikawa2016Document6 pagesMorikawa2016giviNo ratings yet
- Refleksi Kasus VesicolitiasisDocument14 pagesRefleksi Kasus VesicolitiasisgiviNo ratings yet
- Jurnal 3Document13 pagesJurnal 3giviNo ratings yet
- 2 PDFDocument7 pages2 PDFgiviNo ratings yet
- Jurnal GynDocument6 pagesJurnal GyngiviNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Worksheet 8Document2 pagesWorksheet 8Jocel OclaritNo ratings yet
- Olicy: Magna Carta of Public Health Workers: Does It Really Fulfill Its Intent?Document4 pagesOlicy: Magna Carta of Public Health Workers: Does It Really Fulfill Its Intent?Krystal Jane SalinasNo ratings yet
- COVID Testing Labs 26042021Document167 pagesCOVID Testing Labs 26042021suresh10526_71653021No ratings yet
- Test Bank Lehne S Pharmacotherapeutics For Advanced Practice Nurses and Physician Assistants 2nd EdiDocument479 pagesTest Bank Lehne S Pharmacotherapeutics For Advanced Practice Nurses and Physician Assistants 2nd EdiBetsy Brown Byersmith89% (133)
- Soap NoteDocument4 pagesSoap Noteapi-252633788100% (7)
- Xavier BrochureDocument20 pagesXavier BrochureJohn PareraNo ratings yet
- Pathophysiology Schematic Diagram and NarrativeDocument15 pagesPathophysiology Schematic Diagram and NarrativeKathrina CraveNo ratings yet
- Kulit Emergency in DermatologyDocument47 pagesKulit Emergency in DermatologyAulia Shabrina SyukharialNo ratings yet
- Physio For Spondylolisthesis and SpondylolysisDocument12 pagesPhysio For Spondylolisthesis and SpondylolysisHasan RahmanNo ratings yet
- E-Book C Arms-NewDocument9 pagesE-Book C Arms-NewHugoNo ratings yet
- Rogelio Ramos Vs CADocument28 pagesRogelio Ramos Vs CAAnonymous FBDGfUqHENo ratings yet
- As Fluid Volume Deficit (FVD), Hypovolemia) Is ADocument2 pagesAs Fluid Volume Deficit (FVD), Hypovolemia) Is ATanya Alyssa Untalan AquinoNo ratings yet
- PeritonitisDocument21 pagesPeritonitischrisyenNo ratings yet
- Tonetti Et Al-2018-Journal of Periodontology TDocument14 pagesTonetti Et Al-2018-Journal of Periodontology TJonathan Meza MauricioNo ratings yet
- What Are The Reasons For Your Course ChoiceDocument2 pagesWhat Are The Reasons For Your Course Choiceasaad biqaiNo ratings yet
- Proceeding Ilmu KesehatanDocument183 pagesProceeding Ilmu KesehatanIim Rimba100% (1)
- AMSTAR-2 ChecklistDocument10 pagesAMSTAR-2 ChecklistMuammar EmirNo ratings yet
- Case StudyDocument49 pagesCase StudyLennie Marie B Pelaez100% (1)
- Standard Claim Form HospitalDocument2 pagesStandard Claim Form Hospitalnpatel35No ratings yet
- Reflexology Intake FormDocument1 pageReflexology Intake FormJael PistioNo ratings yet
- Atlas of Glaucoma 3E PDFDocument353 pagesAtlas of Glaucoma 3E PDFSUSANA AGUILAR GARCIA100% (1)
- Oman-Guideline On Good Pharmacovigilance PracticesDocument30 pagesOman-Guideline On Good Pharmacovigilance PracticesAmrNo ratings yet
- Customized Devices For OsteosynthesisDocument9 pagesCustomized Devices For OsteosynthesisManas MishraNo ratings yet
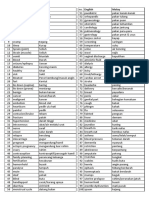
- Medic Term English MalayDocument1 pageMedic Term English MalaySyamimi SuhaimiNo ratings yet
- Stroke Incidence and Case Fatality in AustralasiaDocument7 pagesStroke Incidence and Case Fatality in AustralasiaChintya Anugrah SuhendraNo ratings yet
- SP PaperDocument10 pagesSP Paperapi-506783921No ratings yet
- Pediatric Drug Dosage - All in One PDFDocument15 pagesPediatric Drug Dosage - All in One PDFHuang Hasjim33% (9)
- Pemicu 6 Blok Saraf Dan KejiwaanDocument44 pagesPemicu 6 Blok Saraf Dan KejiwaanTommy WidjajaNo ratings yet
- Program-SUFU 2020 Winter Meeting-2252020Document39 pagesProgram-SUFU 2020 Winter Meeting-2252020Christopher KinsellaNo ratings yet
- Peace Corps Report of Physical Examination - Guide - Att 19 Report of Physical ExaminationDocument6 pagesPeace Corps Report of Physical Examination - Guide - Att 19 Report of Physical ExaminationAccessible Journal Media: Peace Corps DocumentsNo ratings yet