You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A Probability and Statistics CheatsheetDocument28 pagesA Probability and Statistics CheatsheetfarahNo ratings yet
- Enemy Territory - Quake Wars - ManualDocument22 pagesEnemy Territory - Quake Wars - ManualM_MolliNo ratings yet
- Abstract OM NSRC Group 2Document1 pageAbstract OM NSRC Group 2sachin121083No ratings yet
- TQM in An OrganizationDocument83 pagesTQM in An Organizationsachin121083No ratings yet
- Pareto Chart IIDocument11 pagesPareto Chart IIsachin121083No ratings yet
- Analyisis of Location Planning and ExecutionDocument35 pagesAnalyisis of Location Planning and Executionsachin121083No ratings yet
- MFG and Process SelectionDocument12 pagesMFG and Process Selectionsachin121083No ratings yet
- Chapter - 12: ElectricityDocument18 pagesChapter - 12: Electricitysachin121083No ratings yet
- FrameworksDocument21 pagesFrameworkssachin121083100% (1)
- Content: - Definitions of QualityDocument16 pagesContent: - Definitions of Qualitysachin121083No ratings yet
- Cost Reduction of A Product Through Value Analysis Value EngineeringDocument8 pagesCost Reduction of A Product Through Value Analysis Value EngineeringAhmadAl-NafiNo ratings yet
- Facility LocationDocument50 pagesFacility Locationsachin121083No ratings yet
- Subject: TQM and Six Sigma Roll No.Document2 pagesSubject: TQM and Six Sigma Roll No.sachin121083No ratings yet
- Business PlanDocument1 pageBusiness Plansachin121083No ratings yet
- DoeDocument64 pagesDoesachin1210830% (1)
- P ', C - S, - T, Anova: Earson SR HI Quare EST ANDDocument86 pagesP ', C - S, - T, Anova: Earson SR HI Quare EST ANDsachin121083No ratings yet
- Pca IcaDocument34 pagesPca Icasachin121083No ratings yet
- Deckwatchkeeping 1 - Collision RegulationDocument13 pagesDeckwatchkeeping 1 - Collision RegulationLalyn Navora BalansagNo ratings yet
- Handover Process: 1 © NOKIA 1999 Ho - PPT/ July 2000Document50 pagesHandover Process: 1 © NOKIA 1999 Ho - PPT/ July 2000LOCK VALUE3No ratings yet
- Catalogue For AutoDocument22 pagesCatalogue For Autosentimiento azulNo ratings yet
- Diprotic Acid Titration Calculation Worked Example Sulphuric Acid and Sodium Hydroxide - mp4Document2 pagesDiprotic Acid Titration Calculation Worked Example Sulphuric Acid and Sodium Hydroxide - mp4tobiloba temiNo ratings yet
- Feild Inspection of Shell and Tube Heat ExchangersDocument4 pagesFeild Inspection of Shell and Tube Heat ExchangersMatthew BennettNo ratings yet
- Power Quality Standards in ChinaDocument21 pagesPower Quality Standards in ChinaCarlos Talavera VillamarínNo ratings yet
- Applied Hydrology LabDocument6 pagesApplied Hydrology Labshehbaz3gNo ratings yet
- Bricks ComparisonDocument13 pagesBricks ComparisonMd. Numan HossainNo ratings yet
- Pentex Gas OvenDocument5 pagesPentex Gas OvenRahman PashariNo ratings yet
- Motorized Hydraulic PressDocument4 pagesMotorized Hydraulic PressDhiraj Shinde100% (2)
- Manual Multisim 2001 (Ingles)Document72 pagesManual Multisim 2001 (Ingles)Anonymous W1QQcbA4sWNo ratings yet
- SS-7 May Refer To:: RFC 2719 RFC 2719Document15 pagesSS-7 May Refer To:: RFC 2719 RFC 2719William GentryNo ratings yet
- Fifth Wheel, Design and FunctionDocument17 pagesFifth Wheel, Design and FunctionRobert Orosco B.No ratings yet
- ProeDocument160 pagesProejohn100% (1)
- Ee BD ManualDocument37 pagesEe BD Manualsergey62No ratings yet
- Data Warehousing Quick GuideDocument66 pagesData Warehousing Quick Guidejacktheking2010No ratings yet
- Work at Height Questions For Height PassDocument3 pagesWork at Height Questions For Height PassPravash Mohanty100% (1)
- Assimilable Organic Carbon Formation During Ultraviolet - Hydrogen Peroxide Advanced Oxidation Treatment of Surface WaterDocument207 pagesAssimilable Organic Carbon Formation During Ultraviolet - Hydrogen Peroxide Advanced Oxidation Treatment of Surface WaterMonicaRossetimNo ratings yet
- A Review of Power Electronics Based Microgrids: Josep M. Guerrero, Xiongfei Wang, Zhe Chen, and Frede BlaabjergDocument5 pagesA Review of Power Electronics Based Microgrids: Josep M. Guerrero, Xiongfei Wang, Zhe Chen, and Frede BlaabjergSaksham GuptaNo ratings yet
- 07 Power Voltage FeedthroughsDocument52 pages07 Power Voltage FeedthroughsDeepak SomanNo ratings yet
- Samsung E1272 EN PDFDocument2 pagesSamsung E1272 EN PDFmuhammad aslamNo ratings yet
- College ManagementDocument58 pagesCollege Managementforum502No ratings yet
- Lesson 5 T-BeamsDocument7 pagesLesson 5 T-BeamsJoshua John JulioNo ratings yet
- Commercial Office Space - Cyber CityDocument8 pagesCommercial Office Space - Cyber CityankurNo ratings yet
- Stanley 46 InstructionsDocument2 pagesStanley 46 Instructionsj_abendstern4688No ratings yet
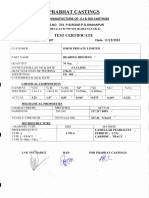
- Omfb MTC 11.12.23Document2 pagesOmfb MTC 11.12.23obviousplatinum2No ratings yet
- Brige Lauching Cap 1 PDFDocument16 pagesBrige Lauching Cap 1 PDFAnonymous VkzquW39No ratings yet
- Code Eac NaceDocument2 pagesCode Eac NaceEvan BuwanaNo ratings yet
- Minimum Load For Empty Minimum Load For OperatingDocument6 pagesMinimum Load For Empty Minimum Load For OperatingjitendraNo ratings yet