You might also like
- Buku SPSS CompleteDocument72 pagesBuku SPSS Completeb6788No ratings yet
- Microsoft Excel Essential Training: Raju Miyan Lecturer Khwopa College of EngineeringDocument25 pagesMicrosoft Excel Essential Training: Raju Miyan Lecturer Khwopa College of EngineeringDipjan ThapaNo ratings yet
- SPSS Commands in STATADocument4 pagesSPSS Commands in STATAShahzad Asghar Arain100% (4)
- Health Technical Memorandum 01-01Document46 pagesHealth Technical Memorandum 01-01O.r. CadzNo ratings yet
- HIV AwarenessDocument35 pagesHIV AwarenessCadine DavisNo ratings yet
- Weekly Epidemiology Report - 5-1-20Document16 pagesWeekly Epidemiology Report - 5-1-20Destiny WashingtonNo ratings yet
- Varicella ZosterDocument41 pagesVaricella Zostertummalapalli venkateswara raoNo ratings yet
- R in Clinical Research and Evidence-Based MedicineDocument376 pagesR in Clinical Research and Evidence-Based MedicineAdrian Olszewski100% (4)
- Multivariate Meta-AnalysisDocument67 pagesMultivariate Meta-AnalysisPantelis BagosNo ratings yet
- Cancer EpidemiologyDocument18 pagesCancer EpidemiologyMariaLisseth MoralesNo ratings yet
- Graphical Displays For Meta-AnalysisDocument15 pagesGraphical Displays For Meta-Analysisdinh son myNo ratings yet
- Chodankar2021 Real World Evidence Vs RCTDocument4 pagesChodankar2021 Real World Evidence Vs RCTMumtaz MaulanaNo ratings yet
- GSR Social Media Research Guidance - Using Social Media For Social ResearchDocument27 pagesGSR Social Media Research Guidance - Using Social Media For Social Researchsophia lorreine chattoNo ratings yet
- Medical Statistics: A Guide to SPSS, Data Analysis and Critical AppraisalFrom EverandMedical Statistics: A Guide to SPSS, Data Analysis and Critical AppraisalNo ratings yet
- Chapter 6 - Statistical Process Control - APIC Text OnlineDocument15 pagesChapter 6 - Statistical Process Control - APIC Text OnlineManalAbdelazizNo ratings yet
- Term Project Analysis of Filter Manufacturing ProcessDocument7 pagesTerm Project Analysis of Filter Manufacturing ProcessUtkarsh Shrivatava0% (1)
- Books on Stata & StatisticsDocument6 pagesBooks on Stata & StatisticsJoeNo ratings yet
- SIS Model For An Infectious DiseaseDocument3 pagesSIS Model For An Infectious DiseaseMohammed AlnasryNo ratings yet
- Leslie D. Rosenstein - Research Design and Analysis - A Primer For The Non-Statistician-John Wiley & Sons (2019)Document253 pagesLeslie D. Rosenstein - Research Design and Analysis - A Primer For The Non-Statistician-John Wiley & Sons (2019)Jorge PereiraNo ratings yet
- The Hot Zone QuestionsDocument8 pagesThe Hot Zone QuestionsGilbert1322No ratings yet
- Acute Flaccid Paralysis: Dr. Madoori SrinivasDocument53 pagesAcute Flaccid Paralysis: Dr. Madoori SrinivasdrravindermehetreyNo ratings yet
- Introduction To Survival Analysis With Stata SeminarDocument16 pagesIntroduction To Survival Analysis With Stata Seminarhubik38No ratings yet
- Course Management SystemDocument5 pagesCourse Management SystemRuchitha GoudNo ratings yet
- Epi in PakistanDocument39 pagesEpi in PakistanJames Smith100% (1)
- Stat AnswersDocument79 pagesStat Answersssckp86No ratings yet
- Survival Analysis in RDocument16 pagesSurvival Analysis in Rmipimipi03No ratings yet
- Surveillance Medical Officer, National Polio Surveillance Project Anywhere in India Indian and International DevelDocument3 pagesSurveillance Medical Officer, National Polio Surveillance Project Anywhere in India Indian and International DevelQuark SupernovaNo ratings yet
- EPI Group 4's History of Immunization ProgramsDocument9 pagesEPI Group 4's History of Immunization Programshaddi awanNo ratings yet
- The U.S. Aviation Safety Reporting SystemDocument7 pagesThe U.S. Aviation Safety Reporting Systemrocklee78No ratings yet
- COVID-19 Future Forecasting Using Supervised Machine Learning ModelsDocument11 pagesCOVID-19 Future Forecasting Using Supervised Machine Learning ModelsOmar DiaaNo ratings yet
- EPI Schedule of PakistanDocument1 pageEPI Schedule of Pakistanksbabar100% (1)
- RM NotesDocument50 pagesRM NotesManu YuviNo ratings yet
- Program Evaluation: Evaluating Civic Engagement Projects (CEPsDocument19 pagesProgram Evaluation: Evaluating Civic Engagement Projects (CEPsjoncan100% (1)
- Syllabus - BiostatisticsDocument3 pagesSyllabus - BiostatisticsJustDen09No ratings yet
- Surveillance of AFPDocument55 pagesSurveillance of AFPsmohisar1100% (3)
- Eradicating Polio in PakistanDocument16 pagesEradicating Polio in PakistanSadammalik2014No ratings yet
- Implementing a Learning Management System at Tarlac State UniversityDocument2 pagesImplementing a Learning Management System at Tarlac State UniversityBong ValdozNo ratings yet
- Challenges Writing Patient Safety NarrativesDocument4 pagesChallenges Writing Patient Safety Narrativessanjeeva reddyNo ratings yet
- Measles SIA Guidelines India - Final - Foreword - Ver3Document122 pagesMeasles SIA Guidelines India - Final - Foreword - Ver3Priscilla Kayina100% (1)
- AFP MigrañaDocument9 pagesAFP MigrañaJuaan AvilaNo ratings yet
- CH 6-2 Comparing Diagnostic TestsDocument8 pagesCH 6-2 Comparing Diagnostic TestsJimmyNo ratings yet
- Okuda-Time Series Analysis of Under-Five MortalityDocument61 pagesOkuda-Time Series Analysis of Under-Five MortalityBoniface Okuda100% (4)
- Iraq Ministry of Health Manual for Acute Flaccid Paralysis SurveillanceDocument29 pagesIraq Ministry of Health Manual for Acute Flaccid Paralysis SurveillanceAuliyaa RahmahNo ratings yet
- Health Literacy QuizDocument6 pagesHealth Literacy QuizSteven GodelmanNo ratings yet
- Lecture 4Document161 pagesLecture 4Jessica AngelinaNo ratings yet
- Getting To Know SPSSDocument204 pagesGetting To Know SPSSTarig GibreelNo ratings yet
- Advice On How To Write A Systematic ReviewDocument12 pagesAdvice On How To Write A Systematic ReviewDibyendunarayan Bid100% (1)
- Producs Laboratory Shift Table PDFDocument10 pagesProducs Laboratory Shift Table PDFarrarrgee8005No ratings yet
- Module 5 - Ordinal RegressionDocument55 pagesModule 5 - Ordinal RegressionMy Hanh DoNo ratings yet
- Practical Missing Data Analysis in SPSSDocument19 pagesPractical Missing Data Analysis in SPSSlphouneNo ratings yet
- Mymodules Unisa 2015Document388 pagesMymodules Unisa 2015RixizoNgobeni67% (3)
- Fit Indices Commonly Reported For CFA and SEMDocument2 pagesFit Indices Commonly Reported For CFA and SEMAbhinav NigamNo ratings yet
- Intro Biostats GuideDocument16 pagesIntro Biostats GuideMinhao Hu100% (1)
- MYCINDocument5 pagesMYCINsaurabh3112vermaNo ratings yet
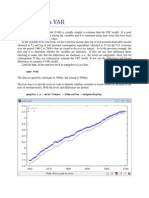
- Estimating a VAR Model in GRETLDocument9 pagesEstimating a VAR Model in GRETLkaddour7108No ratings yet
- CM304Document25 pagesCM304api-3849444No ratings yet
- N4325 AP EBP Project - Finding The EvidenceDocument6 pagesN4325 AP EBP Project - Finding The Evidencemeow_meow163100% (1)
- Estimation of Sample SizeDocument33 pagesEstimation of Sample SizekhoafnnNo ratings yet
- Handbook Bio StatDocument305 pagesHandbook Bio StatADWINDT100% (1)
- Pantry Evaluation Proposal InternshipDocument6 pagesPantry Evaluation Proposal Internshipapi-293251016No ratings yet
- OrdinalexampleR PDFDocument9 pagesOrdinalexampleR PDFDamon CopelandNo ratings yet
- Multidimensional Mathematical Demography: Proceedings of the Conference on Multidimensional Mathematical Demography Held at the University of Maryland, College Park, Maryland, March 23-25, 1981, Sponsored by the National Science FoundationFrom EverandMultidimensional Mathematical Demography: Proceedings of the Conference on Multidimensional Mathematical Demography Held at the University of Maryland, College Park, Maryland, March 23-25, 1981, Sponsored by the National Science FoundationNo ratings yet
- Modified Alvarado Score and Its Application in The Diagnosis of Acute AppendicitisDocument2 pagesModified Alvarado Score and Its Application in The Diagnosis of Acute AppendicitisanunadNo ratings yet
- Modified Alvarado Score and Its Application in The Diagnosis of Acute AppendicitisDocument3 pagesModified Alvarado Score and Its Application in The Diagnosis of Acute AppendicitisnucaiceNo ratings yet
- 2.operational Guidelines DEIC RBSKDocument100 pages2.operational Guidelines DEIC RBSKChristopher Mala100% (1)
- Operational Guidelines RBSKDocument43 pagesOperational Guidelines RBSKanunad100% (1)
- National Vaccine Policy BookDocument23 pagesNational Vaccine Policy BookbajrangiNo ratings yet
- Pentavalent Vaccine Operational Guidelines 2013Document36 pagesPentavalent Vaccine Operational Guidelines 2013anunadNo ratings yet
- Immunization M 4 SupervisionDocument49 pagesImmunization M 4 SupervisionanunadNo ratings yet
- IDCF Guidelines 2016Document47 pagesIDCF Guidelines 2016anunad100% (2)
- Prep Guidelines UpdatedDocument54 pagesPrep Guidelines UpdatedHeartful charltonNo ratings yet
- Daftar Harga Vaksinasi Oktober 2022Document1 pageDaftar Harga Vaksinasi Oktober 2022IF RS Surya AsihNo ratings yet
- Varicella Vaccine Information Sheet: WWW - Vaccinesafety.edu/porcine-Vaccineapproval - HTMDocument2 pagesVaricella Vaccine Information Sheet: WWW - Vaccinesafety.edu/porcine-Vaccineapproval - HTMdini fitriastutiNo ratings yet
- 2021 VAERS Vaccine Type As of 4/2/2021Document2,342 pages2021 VAERS Vaccine Type As of 4/2/2021PJ MediaNo ratings yet
- Condom UseDocument2 pagesCondom UseMuhamad FakhrullahNo ratings yet
- 1425 25 2628 1 10 20200518 DikonversiDocument7 pages1425 25 2628 1 10 20200518 DikonversiErna YulianaNo ratings yet
- Measles CIF 2014Document2 pagesMeasles CIF 2014RionaMarieMagbutayNo ratings yet
- Annex A and B For Dengvaxia ProfilingDocument3 pagesAnnex A and B For Dengvaxia ProfilingAnne 닌 야 PiedadNo ratings yet
- Health Belief Model on Dengue Fever PatientsDocument10 pagesHealth Belief Model on Dengue Fever PatientsPaulina PakpahanNo ratings yet
- Laporan Obat Sesuai Foemularium Februari 2019Document24 pagesLaporan Obat Sesuai Foemularium Februari 2019Maria AmabiNo ratings yet
- RECORDING Form 1: Masterlist of Students Masterlist of Kinder 1 To Grade 7 (Except Grade 4)Document7 pagesRECORDING Form 1: Masterlist of Students Masterlist of Kinder 1 To Grade 7 (Except Grade 4)Rainel ManosNo ratings yet
- BHHP 7-9 PDFDocument1 pageBHHP 7-9 PDFSiti MasturaNo ratings yet
- Prinsipal: PT. Biofarma: Pt. Merapi Utama Pharma Daftar Harga Berlaku: 4 Januari 2021Document3 pagesPrinsipal: PT. Biofarma: Pt. Merapi Utama Pharma Daftar Harga Berlaku: 4 Januari 2021AtmaNo ratings yet
- Causes and clinical features of oral lesionsDocument6 pagesCauses and clinical features of oral lesionsAbdullah Misini100% (1)
- Chickenpox (Varicella) : What Is Chickenpox? What Are The Symptoms of Chickenpox?Document3 pagesChickenpox (Varicella) : What Is Chickenpox? What Are The Symptoms of Chickenpox?Helga Yoan Ladymeyer TimbayoNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination DetailsShasha BakarNo ratings yet
- File, 4285, enDocument2 pagesFile, 4285, enAfra FitrianitaNo ratings yet
- Everything You Need to Know About ChickenpoxDocument10 pagesEverything You Need to Know About ChickenpoxNessa Layos MorilloNo ratings yet
- Understanding HIV/AIDSDocument2 pagesUnderstanding HIV/AIDSMbiatat BrandonNo ratings yet
- BrochureGroup 1Document2 pagesBrochureGroup 1classdocsNo ratings yet
- Infections:: Jadwal Acara Pelatihan In-Alarm Hari II: Minggu, 28 Februari 2021 Waktu Menit Acara Pembicara AbsensiDocument1 pageInfections:: Jadwal Acara Pelatihan In-Alarm Hari II: Minggu, 28 Februari 2021 Waktu Menit Acara Pembicara AbsensiClarestaNo ratings yet
- Interpretation: L55 - PSC Jayanagar Home Visit Municipal New No.42, Old No 825, Ground, W K P Road, 7Th Block, JayanagarDocument2 pagesInterpretation: L55 - PSC Jayanagar Home Visit Municipal New No.42, Old No 825, Ground, W K P Road, 7Th Block, JayanagardrmohangNo ratings yet
- Concept Map Group 1Document1 pageConcept Map Group 1eric macabiog100% (1)
- Rubella: Causes, Symptoms and PreventionDocument19 pagesRubella: Causes, Symptoms and PreventionRiya KayarkarNo ratings yet
- ZIM ART Guidelines 2016 - Review FinalDocument136 pagesZIM ART Guidelines 2016 - Review FinalCollen LihakaNo ratings yet
- Young Mothers' HIV/AIDS Prevention Knowledge, Attitudes, and PracticesDocument11 pagesYoung Mothers' HIV/AIDS Prevention Knowledge, Attitudes, and PracticesSITI MONAUWARAH BT MOKHTARNo ratings yet
- Maureen Chilila, Jhpiego-Zambia, IAS 2012 Poster, Couple CounselingDocument1 pageMaureen Chilila, Jhpiego-Zambia, IAS 2012 Poster, Couple CounselingJhpiegoNo ratings yet