You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Secondary CarotenemiaDocument3 pagesSecondary CarotenemiaMedrechEditorialNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hayling Test: Development and Normalization of The Spanish VersionDocument9 pagesThe Hayling Test: Development and Normalization of The Spanish VersionMariaNo ratings yet
- Zelazo 2013 Oxford Handbook Developmental Psychology Vol. 1 PDFDocument1,285 pagesZelazo 2013 Oxford Handbook Developmental Psychology Vol. 1 PDFlicanthroppe80% (5)
- Mind Wide Open 2004 EbookDocument98 pagesMind Wide Open 2004 EbookEric Shaydullin100% (4)
- Giant Cell ReparativeDocument3 pagesGiant Cell ReparativeMedrechEditorialNo ratings yet
- How Stupid Is Google Making UsDocument4 pagesHow Stupid Is Google Making Ustoamyp100% (1)
- Textbook Geriatric Psychiatry 09 PDFDocument23 pagesTextbook Geriatric Psychiatry 09 PDFLydia AmaliaNo ratings yet
- Assessment of Human Papilloma VirusDocument11 pagesAssessment of Human Papilloma VirusMedrechEditorialNo ratings yet
- Type 2 Diabetes With RecurrentDocument5 pagesType 2 Diabetes With RecurrentMedrechEditorialNo ratings yet
- Post Operative Visual Outcome in MultifocalDocument6 pagesPost Operative Visual Outcome in MultifocalMedrechEditorialNo ratings yet
- Traumatic Brain Injury in AdultsDocument11 pagesTraumatic Brain Injury in AdultsMedrechEditorialNo ratings yet
- Unusual Lung Involvement With EchinococcusDocument5 pagesUnusual Lung Involvement With EchinococcusMedrechEditorialNo ratings yet
- The Correlation BetweenDocument6 pagesThe Correlation BetweenMedrechEditorialNo ratings yet
- 181 Study of The Clinical Profile of PatientsDocument5 pages181 Study of The Clinical Profile of PatientsMedrechEditorialNo ratings yet
- Biofilm Production Among BacterialDocument7 pagesBiofilm Production Among BacterialMedrechEditorialNo ratings yet
- An Investigation and Management ofDocument9 pagesAn Investigation and Management ofMedrechEditorialNo ratings yet
- 187 Manual Nuclear Division in Anterior Chamber PDFDocument7 pages187 Manual Nuclear Division in Anterior Chamber PDFMedrechEditorialNo ratings yet
- Comparison of The Effect ofDocument8 pagesComparison of The Effect ofMedrechEditorialNo ratings yet
- The White Plan and Hospital Resilience TwoDocument12 pagesThe White Plan and Hospital Resilience TwoMedrechEditorialNo ratings yet
- Results of Penetrating KeratoplastyDocument9 pagesResults of Penetrating KeratoplastyMedrechEditorialNo ratings yet
- Estimation of Serum Ferritin Level of A CohortDocument5 pagesEstimation of Serum Ferritin Level of A CohortMedrechEditorialNo ratings yet
- Chronic Non-SpecificDocument8 pagesChronic Non-SpecificMedrechEditorialNo ratings yet
- Suspiciuos But Sudden Cardiovascular DeathsDocument5 pagesSuspiciuos But Sudden Cardiovascular DeathsMedrechEditorialNo ratings yet
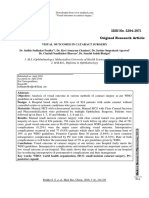
- Visual Outcomes inDocument18 pagesVisual Outcomes inMedrechEditorialNo ratings yet
- Abdominal Trauma and Brain InjuryyyyDocument12 pagesAbdominal Trauma and Brain InjuryyyyMedrechEditorialNo ratings yet
- A Year Review of SuspectedDocument5 pagesA Year Review of SuspectedMedrechEditorialNo ratings yet
- Comparing The Spiritual Care View PointDocument9 pagesComparing The Spiritual Care View PointMedrechEditorialNo ratings yet
- Preoperatice AcDocument5 pagesPreoperatice AcMedrechEditorialNo ratings yet
- 213 Organizing To Meet Critical Needs For MaternitooDocument8 pages213 Organizing To Meet Critical Needs For MaternitooMedrechEditorialNo ratings yet
- The Incidence RateDocument7 pagesThe Incidence RateMedrechEditorialNo ratings yet
- New Innovation in Endodontic TherapyDocument4 pagesNew Innovation in Endodontic TherapyMedrechEditorialNo ratings yet
- Serum ErythropoietinDocument8 pagesSerum ErythropoietinMedrechEditorialNo ratings yet
- Subcutaneous Emphysema and Mandibular ThirdDocument4 pagesSubcutaneous Emphysema and Mandibular ThirdMedrechEditorialNo ratings yet
- Tuberculosis Unmasks Myasthenia - ADocument4 pagesTuberculosis Unmasks Myasthenia - AMedrechEditorialNo ratings yet
- Empirical evidence supports higher-order consciousness theoriesDocument9 pagesEmpirical evidence supports higher-order consciousness theorieskarlunchoNo ratings yet
- Macaca Fascicularis: Pattern of Novel Object Exploration in Cynomolgus MonkeyDocument7 pagesMacaca Fascicularis: Pattern of Novel Object Exploration in Cynomolgus MonkeyEsteli189No ratings yet
- Chun CONB 2007Document8 pagesChun CONB 2007j00000000No ratings yet
- Depression in Neurodegenerative Diseases - Common Mechanisms and Current Treatment OptionsDocument103 pagesDepression in Neurodegenerative Diseases - Common Mechanisms and Current Treatment OptionsAna Paula LopesNo ratings yet
- Where Does The Brain Store Long-Ago Memories - Scientific AmericanDocument4 pagesWhere Does The Brain Store Long-Ago Memories - Scientific AmericanlmrocesNo ratings yet
- Paul Allen@roehampton Ac UkDocument22 pagesPaul Allen@roehampton Ac UkGetha ManuabaNo ratings yet
- Adele DiamondsDocument5 pagesAdele Diamondsgina1975No ratings yet
- Neural substrates of cognitive flexibility linked to preschool irritabilityDocument7 pagesNeural substrates of cognitive flexibility linked to preschool irritabilityRatna Ayu WulandariNo ratings yet
- Mindfulness Training and Neural Integration: Differentiation of Distinct Streams of Awareness and The Cultivation of Well-BeingDocument5 pagesMindfulness Training and Neural Integration: Differentiation of Distinct Streams of Awareness and The Cultivation of Well-BeingGretchen Marie Aristud AquinoNo ratings yet
- Neuroawakening PDFDocument13 pagesNeuroawakening PDFMartin Martinez RiveraNo ratings yet
- FNIRS2018 AbstractDocument312 pagesFNIRS2018 AbstractJn5omEghSU0j0FNo ratings yet
- Predict Motor Learning EEGDocument29 pagesPredict Motor Learning EEGwidyarnia17No ratings yet
- Inhibitory Control Over Action and MemoryDocument11 pagesInhibitory Control Over Action and MemoryMaryam TaqaviNo ratings yet
- Wimh Winter 2010 WebDocument4 pagesWimh Winter 2010 WebNick LuchettiNo ratings yet
- Special Issue Therapeutic Benefits of Physical Activity For Mood A Systematic Review On The Effects of Exercise Intensity Duration and ModalityDocument25 pagesSpecial Issue Therapeutic Benefits of Physical Activity For Mood A Systematic Review On The Effects of Exercise Intensity Duration and ModalityjasonNo ratings yet
- Godefroy PDFDocument6 pagesGodefroy PDFMaria georgianaNo ratings yet
- The Emotional Life of Your Brain: Richard DavidsonDocument18 pagesThe Emotional Life of Your Brain: Richard DavidsonBegüm GüvenNo ratings yet
- Neuropsychologia: Thomas Goschke, Annette BolteDocument21 pagesNeuropsychologia: Thomas Goschke, Annette BolteFrancisco Ahumada MéndezNo ratings yet
- Measuring Spontaneous Processes in CreativityDocument7 pagesMeasuring Spontaneous Processes in CreativitySarah KazmiNo ratings yet
- Neuroscientific and Behavioral Genetic Information in Criminal Cases in The NetherlandsDocument26 pagesNeuroscientific and Behavioral Genetic Information in Criminal Cases in The NetherlandsFrixos StephanidesNo ratings yet
- Prefrontal Deep Projection Neurons Enable Cognitive Flexibility Via Persistent Feedback Monitoring PDFDocument35 pagesPrefrontal Deep Projection Neurons Enable Cognitive Flexibility Via Persistent Feedback Monitoring PDFHelping OthersNo ratings yet
- Psychological Well Being Evidence Regarding Its Causes and ConsequencesDocument28 pagesPsychological Well Being Evidence Regarding Its Causes and Consequencesarya atmawijayaNo ratings yet
- Cognitive Behavioral Therapy For Schizophrenia An Overview On Efficacy Recent Trends and Neurobiological FindingsDocument10 pagesCognitive Behavioral Therapy For Schizophrenia An Overview On Efficacy Recent Trends and Neurobiological FindingsKaplan GenadiNo ratings yet
- NEUR3502 Lectures 11Document27 pagesNEUR3502 Lectures 11Ryan HiraniNo ratings yet
- Psychology Dissertation Research TopicsDocument7 pagesPsychology Dissertation Research TopicsHelpWritingPapersSingapore100% (1)