You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Daftar Obat Puskes MerdekaDocument2 pagesDaftar Obat Puskes MerdekaAnonymous aH8gCZ7zjNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
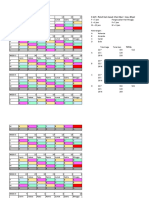
- 3 Shift: Pola 3 Hari Masuk 1 Hari Libur + Max. 40 Jam/mingguDocument4 pages3 Shift: Pola 3 Hari Masuk 1 Hari Libur + Max. 40 Jam/mingguAnonymous aH8gCZ7zjNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Research Article: Characterization of Pediatric Acute Lymphoblastic Leukemia Survival Patterns by Age at DiagnosisDocument10 pagesResearch Article: Characterization of Pediatric Acute Lymphoblastic Leukemia Survival Patterns by Age at DiagnosisAnonymous aH8gCZ7zjNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Case HemoroidDocument19 pagesCase HemoroidAnonymous aH8gCZ7zjNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- ID Hubungan Faktor Resiko Dengan Terjadinya Nyeri Punggung Bawah Low Back Pain Pada PDFDocument10 pagesID Hubungan Faktor Resiko Dengan Terjadinya Nyeri Punggung Bawah Low Back Pain Pada PDFAnonymous aH8gCZ7zjNo ratings yet
- IT 3 - Spinal Cord InjuryDocument38 pagesIT 3 - Spinal Cord InjuryAnonymous aH8gCZ7zjNo ratings yet
- Excercise 2 - Frequency MeasureDocument6 pagesExcercise 2 - Frequency MeasureAnonymous aH8gCZ7zj75% (4)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Etails Hits: 13657: Municipal Ordinance No. 12-233Document18 pagesEtails Hits: 13657: Municipal Ordinance No. 12-233Dianne MacaraigNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Gambang SmoDocument4 pagesGambang SmoAlvin ComilaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Health Situational AnalysisDocument70 pagesHealth Situational AnalysisGretchen Mae Corrales100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Safe MotherhoodDocument27 pagesSafe MotherhoodEsory BasnetNo ratings yet
- BEmONC - Facilitator's Handbook - 2013 April - FinalDocument286 pagesBEmONC - Facilitator's Handbook - 2013 April - FinalElizabeth Nionzima100% (2)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Who-Safe Childbirth Checklist Implementation GuideDocument62 pagesWho-Safe Childbirth Checklist Implementation GuideMamalia RamadaniNo ratings yet
- 03chapter4 PDFDocument72 pages03chapter4 PDFAnonymous bT8Fs8daY2No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Safe Motherhood Ordinance 2011Document17 pagesSafe Motherhood Ordinance 2011Dhonnalyn Amene Caballero100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- NHSRC - Operational Guidelines On Maternal and Newborn HealthDocument46 pagesNHSRC - Operational Guidelines On Maternal and Newborn HealthNational Child Health Resource Centre (NCHRC)No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Iloilo City Regulation Ordinance 2015-163Document5 pagesIloilo City Regulation Ordinance 2015-163Iloilo City CouncilNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Form No.1 Birth ReportDocument4 pagesForm No.1 Birth ReportSruthy SasiNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- O12824-2014 (Providing For The Safe Motherhood)Document5 pagesO12824-2014 (Providing For The Safe Motherhood)CdeoCityCouncil100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Municipal Ordinance No. 04-2012Document6 pagesMunicipal Ordinance No. 04-2012JayPardinianNuyda100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Skilled Birth AttendantDocument33 pagesSkilled Birth Attendantvkb_99996326No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)