You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Palpitations AND Heartbeat Disorders: By: Aisha Sara Tasnim Physician: DR SsebulibaDocument22 pagesPalpitations AND Heartbeat Disorders: By: Aisha Sara Tasnim Physician: DR SsebulibaNinaNo ratings yet
- SeminarDocument34 pagesSeminarMuhammad Faiz Satria WibowoNo ratings yet
- Roth 12618 BSGM ReportDocument35 pagesRoth 12618 BSGM ReportWhite DiamondNo ratings yet
- Hypertension Testing GuidelinesDocument129 pagesHypertension Testing GuidelinesChunlei WangNo ratings yet
- Boston Scientific Watchman Coverage DecisionDocument124 pagesBoston Scientific Watchman Coverage DecisionmedtechyNo ratings yet
- ECG StripsDocument5 pagesECG Stripssurviving nursing school100% (1)
- FADocument8 pagesFALupita GutierrezNo ratings yet
- Answers MediDocument443 pagesAnswers MediAmine Younis100% (13)
- 3 - Assigned-Cases-09 26 20Document112 pages3 - Assigned-Cases-09 26 20janna cavalesNo ratings yet
- GuidelinesDocument4 pagesGuidelinesChidambaram SeevakanNo ratings yet
- Management of ACSDocument46 pagesManagement of ACSsanjeevNo ratings yet
- Group 4 Thyroid Storm ALADocument25 pagesGroup 4 Thyroid Storm ALAJessica RamosNo ratings yet
- Bridging Anticoagulation JACC 2015Document12 pagesBridging Anticoagulation JACC 2015Frans LiwangNo ratings yet
- Afib Simplified Guidelines Treatment Chart UCM - 324032 PDFDocument1 pageAfib Simplified Guidelines Treatment Chart UCM - 324032 PDFLakshay TyagiNo ratings yet
- Scientific Programme 18th APCC 090311Document33 pagesScientific Programme 18th APCC 090311drsmiNo ratings yet
- Resident Survival GuideDocument104 pagesResident Survival Guidescalixto100% (1)
- ECG Rhythm Strip Interpretation Lesson 4Document5 pagesECG Rhythm Strip Interpretation Lesson 4phoebjaetanNo ratings yet
- Atria Risk Score - Jaha 2013Document11 pagesAtria Risk Score - Jaha 2013LR NesNo ratings yet
- RevisionDocument17 pagesRevisionMatt RenaudNo ratings yet
- DR Erwin Sukandi, SPPD, K-KV BelumDocument47 pagesDR Erwin Sukandi, SPPD, K-KV BelumrajaalfatihNo ratings yet
- Atrial FibrillationDocument252 pagesAtrial FibrillationyurikhanNo ratings yet
- Patient Education ToolkitDocument14 pagesPatient Education ToolkitI Nyoman Gede SemarajanaNo ratings yet
- Supraventricular Arrhythmias (Seminar)Document29 pagesSupraventricular Arrhythmias (Seminar)Muvenn KannanNo ratings yet
- Abnormal EcgDocument6 pagesAbnormal EcgYash Raj SisodiyaNo ratings yet
- Mobile Health Technology Supported Atrial Fibrillation S - 2020 - European JournDocument7 pagesMobile Health Technology Supported Atrial Fibrillation S - 2020 - European JournStefan LaurentiuNo ratings yet
- Report-Ecg Ctscan G3 Friday PDFDocument25 pagesReport-Ecg Ctscan G3 Friday PDFTrí Tạ MinhNo ratings yet
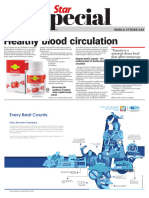
- World Stroke Day - 29 October 2023Document5 pagesWorld Stroke Day - 29 October 2023Times MediaNo ratings yet
- HypomagnesemiaDocument3 pagesHypomagnesemiaapi-3712326No ratings yet
- Jama Kamel 2024 Oi 230163 1706898479.89128Document9 pagesJama Kamel 2024 Oi 230163 1706898479.89128Srinivas PingaliNo ratings yet
- Bogdan A. Popescu: University of Medicine and Pharmacy Bucharest, RomaniaDocument37 pagesBogdan A. Popescu: University of Medicine and Pharmacy Bucharest, RomaniaSolaris_movementNo ratings yet