You might also like
- Serous Fluids: DMT 4206 Group ThreeDocument55 pagesSerous Fluids: DMT 4206 Group ThreePyneandy KimberlyNo ratings yet
- Transudate or ExudateDocument6 pagesTransudate or ExudateDattatreyaNo ratings yet
- Exudate: Transudates Are Caused by Disturbances of Hydrostatic or Colloid Osmotic Pressure, NotDocument3 pagesExudate: Transudates Are Caused by Disturbances of Hydrostatic or Colloid Osmotic Pressure, NotAdnan LiaqatNo ratings yet
- Body FluidsDocument24 pagesBody FluidsMohamed MidoNo ratings yet
- Fecal Analisys: Evi Puspita SariDocument17 pagesFecal Analisys: Evi Puspita Sarisepti dwi andiniNo ratings yet
- Diagnostic TestingDocument112 pagesDiagnostic TestingAbdullah AbsaniNo ratings yet
- Transudate vs. Exudate OverviewDocument4 pagesTransudate vs. Exudate OverviewAdam LechnerNo ratings yet
- Body Fluids (Final)Document31 pagesBody Fluids (Final)Fatima ZuhraNo ratings yet
- Serous Fluids AnalysisDocument15 pagesSerous Fluids AnalysisMustafa Khandgawi100% (1)
- 9.0 Blood AnalysisDocument11 pages9.0 Blood Analysiskibitokstephen1No ratings yet
- Urine AnalysisDocument43 pagesUrine AnalysisBayan MahmoudNo ratings yet
- Serous FluidDocument42 pagesSerous FluidLian Marie ViñasNo ratings yet
- Cytology of Body FluidDocument68 pagesCytology of Body FluidZeeshan YousufNo ratings yet
- Pleural FluidDocument2 pagesPleural FluidNatasha Mae BenitezNo ratings yet
- Blood AnalysisDocument10 pagesBlood AnalysisHry WkNo ratings yet
- RMU Session 7 - Diagnostic Support and EBMDocument40 pagesRMU Session 7 - Diagnostic Support and EBMgatete samNo ratings yet
- Macroscopic UrinalysisDocument29 pagesMacroscopic UrinalysisJames De VeraNo ratings yet
- Diagnositc Testing: By: Jervy P. Beranrdino, RN, MSNDocument34 pagesDiagnositc Testing: By: Jervy P. Beranrdino, RN, MSNadni_wgNo ratings yet
- AtlasDocument8 pagesAtlasPatricia MendozaNo ratings yet
- CLM IiDocument24 pagesCLM IiKuma BelloNo ratings yet
- Blood Test PresentationDocument129 pagesBlood Test Presentationනුවන් චමීර ගුණවර්ධනNo ratings yet
- Iii. Laboratory and Diagnostic Examinations Hematology October 24, 2014 Examination Result Normal Values InterpretationDocument22 pagesIii. Laboratory and Diagnostic Examinations Hematology October 24, 2014 Examination Result Normal Values InterpretationDizerine Mirafuentes RolidaNo ratings yet
- Synovial FluidDocument19 pagesSynovial FluidLian Marie ViñasNo ratings yet
- Lab ValuesDocument60 pagesLab ValuesTatyanna RammouzNo ratings yet
- Introduction To Clinical ChemistryDocument12 pagesIntroduction To Clinical ChemistryNada hasan91% (11)
- Laboratory Testing and Cytology of Serous FluidsDocument48 pagesLaboratory Testing and Cytology of Serous FluidsJohn Reden RomeroNo ratings yet
- 12 Serous Fluid Analysis STUDENTDocument24 pages12 Serous Fluid Analysis STUDENTrbm121415chyNo ratings yet
- UrineDocument52 pagesUrineMohammed Tahoun100% (1)
- Diagnostic Procedures Final 1Document4 pagesDiagnostic Procedures Final 1Nina MoradaNo ratings yet
- Limulus Amebocyte Lysate Test (LAL)Document16 pagesLimulus Amebocyte Lysate Test (LAL)Shahriar ShamimNo ratings yet
- Normal Laboratory ValuesDocument40 pagesNormal Laboratory ValuesPrincess Nasima M. Usngan100% (1)
- Clinical Pathology Fecalysis and UrnalysisDocument16 pagesClinical Pathology Fecalysis and UrnalysisRem Alfelor100% (3)
- Physical Examination of Urine: Analysis of Urine and Other Body Fluids Module 4Document19 pagesPhysical Examination of Urine: Analysis of Urine and Other Body Fluids Module 4Francis ValdezNo ratings yet
- Introduction and Interference NewDocument24 pagesIntroduction and Interference Newkholoud220No ratings yet
- Blood Presentation SV Sp16Document36 pagesBlood Presentation SV Sp16LuisNovelo12No ratings yet
- Clinical MicrosDocument20 pagesClinical MicrosKG CubilNo ratings yet
- Cirulatory System BloodDocument86 pagesCirulatory System BloodAyeshaNo ratings yet
- Laboratory Result: Normal AbnormalDocument3 pagesLaboratory Result: Normal AbnormalMartin T ManuelNo ratings yet
- Chapter 9 PPT ON BLOODDocument33 pagesChapter 9 PPT ON BLOODRicojohn ManimtimNo ratings yet
- Summary of Normal Laboratory ValuesDocument24 pagesSummary of Normal Laboratory ValuesMissy U. TorrechillaNo ratings yet
- Paracentesis: Analysate InterpretationDocument2 pagesParacentesis: Analysate InterpretationNor Ubudiah SetiNo ratings yet
- Stool ExaminationDocument82 pagesStool Examinationambadepravin100% (2)
- Decena, Cyrille Justine A. BSN-4A: Competency AppraisalDocument4 pagesDecena, Cyrille Justine A. BSN-4A: Competency AppraisalJohn Glenn Balacano100% (2)
- Hematology PPT 1Document287 pagesHematology PPT 1TarishiMalikNo ratings yet
- Biological Fluids & Urine Analysis Lec 1Document62 pagesBiological Fluids & Urine Analysis Lec 1Ayman SaberNo ratings yet
- Lab - AGE CaseDocument7 pagesLab - AGE CaseDenice Ann Barboza-MahiposNo ratings yet
- Urine and Feces ExaminationsDocument36 pagesUrine and Feces Examinationsshubhamthakurst1108No ratings yet
- UrineDocument17 pagesUrinealynne_pascua8530No ratings yet
- Clinical Microscopy:: Case Study AnalysisDocument12 pagesClinical Microscopy:: Case Study Analysischocoholic potchiNo ratings yet
- Lab TestDocument7 pagesLab TestNIKKI JOYCE PASIANNo ratings yet
- English Comp Urinalysis Mdb-AnalytesDocument15 pagesEnglish Comp Urinalysis Mdb-AnalytesTrini PurnamasariNo ratings yet
- Lesson 3 FORENSIC SEROLOGY Blood Stain ExaminationDocument23 pagesLesson 3 FORENSIC SEROLOGY Blood Stain ExaminationEzekiel MarinoNo ratings yet
- Chapter Four: Chemical Analysis of UrineDocument174 pagesChapter Four: Chemical Analysis of UrineRebuma BeleteNo ratings yet
- Urinalysis - Chemical, Physical and Microscopic Examination of UrineDocument6 pagesUrinalysis - Chemical, Physical and Microscopic Examination of UrineGaurav KatariaNo ratings yet
- Blood Test RangesDocument18 pagesBlood Test Rangeskltran80No ratings yet
- Blood Test: For The Novel by Jonathan Kellerman, SeeDocument7 pagesBlood Test: For The Novel by Jonathan Kellerman, SeeMaharani IndriNo ratings yet
- Final Laboratory ProceduresDocument14 pagesFinal Laboratory ProceduresJosh BlasNo ratings yet
- Interpretation of Urine DRDocument117 pagesInterpretation of Urine DRShanza AmaanNo ratings yet
- Drug StudyDocument11 pagesDrug StudyMichelle TamorNo ratings yet
- Activity Sheet 1 IntroductionDocument5 pagesActivity Sheet 1 IntroductionMichelle TamorNo ratings yet
- Final Discharge PlanDocument4 pagesFinal Discharge PlanMichelle TamorNo ratings yet
- Muscular System Anatomy and PhysiologyDocument9 pagesMuscular System Anatomy and PhysiologyMichelle Tamor100% (1)
- Shirt FontDocument3 pagesShirt FontMichelle TamorNo ratings yet
- Muscular System Anatomy and PhysiologyDocument9 pagesMuscular System Anatomy and PhysiologyMichelle Tamor100% (1)
- 20 Increment 52week Money ChallengeDocument2 pages20 Increment 52week Money ChallengeMichelle TamorNo ratings yet
- PEEEEEEEEEEEEEEEDocument2 pagesPEEEEEEEEEEEEEEEMichelle TamorNo ratings yet
- PerfDocument1 pagePerfMichelle TamorNo ratings yet
- Orthopedic NursingDocument2 pagesOrthopedic NursingMichelle TamorNo ratings yet
- Nursing Care Analysis Record: Rosemarie Carreon ReyesDocument35 pagesNursing Care Analysis Record: Rosemarie Carreon ReyesMichelle TamorNo ratings yet
- ErcpDocument4 pagesErcpMichelle TamorNo ratings yet
- Case Study - Part 2Document9 pagesCase Study - Part 2Michelle TamorNo ratings yet
- Drug StudyDocument4 pagesDrug StudyMichelle TamorNo ratings yet
- Chron's DiseaseDocument9 pagesChron's DiseaseMichelle TamorNo ratings yet
- NCPDocument3 pagesNCPMichelle TamorNo ratings yet
- DOHStat - Health Status-Notifiable DiseasesDocument17 pagesDOHStat - Health Status-Notifiable DiseasesEber AmadeusNo ratings yet
- Basic AnatomyDocument26 pagesBasic AnatomyMichelle TamorNo ratings yet
- Care of Clients Requiring SurgeryDocument4 pagesCare of Clients Requiring SurgeryMichelle Tamor100% (1)
- Orthopedic NursingDocument2 pagesOrthopedic NursingMichelle TamorNo ratings yet
- The Premier Medical Center Bloodletting ProgramDocument1 pageThe Premier Medical Center Bloodletting ProgramMichelle TamorNo ratings yet
- Raynauds DiseaseDocument15 pagesRaynauds DiseaseMichelle TamorNo ratings yet
- FractureDocument2 pagesFractureMichelle TamorNo ratings yet
- Laboratories: HEMATOLOGY - January 31, 2017 Normal Values Result SignificanceDocument2 pagesLaboratories: HEMATOLOGY - January 31, 2017 Normal Values Result SignificanceMichelle TamorNo ratings yet
- Irritable Bowel Syndrome (Ibs)Document6 pagesIrritable Bowel Syndrome (Ibs)Michelle TamorNo ratings yet
- Bronchiectasis: Prepared By: Michelle TamorDocument17 pagesBronchiectasis: Prepared By: Michelle TamorMichelle TamorNo ratings yet
- Folic Acid Deficiency AnemiaDocument8 pagesFolic Acid Deficiency AnemiaMichelle TamorNo ratings yet
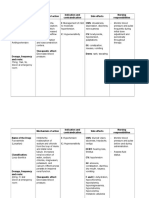
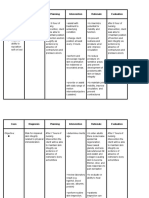
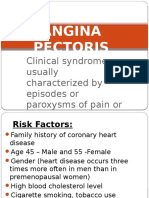
- Angina PectorisDocument8 pagesAngina PectorisMichelle TamorNo ratings yet
- Myocardial Infarction: Refers To The Process by Which Areas of Myocardial Cells in The Heart Are Permanently DestroyedDocument7 pagesMyocardial Infarction: Refers To The Process by Which Areas of Myocardial Cells in The Heart Are Permanently DestroyedMichelle TamorNo ratings yet
- Delfi Spec LimbProtectionSleeveDocument2 pagesDelfi Spec LimbProtectionSleeveabhishekbmcNo ratings yet
- What Are The Health Benefits of Soy?Document4 pagesWhat Are The Health Benefits of Soy?Irfan SuliansyahNo ratings yet
- Earth and Life Science Week 14 (Perpetuation of Life) : DECEMBER 1-4, 2020Document9 pagesEarth and Life Science Week 14 (Perpetuation of Life) : DECEMBER 1-4, 2020Ann Kyla ManrezaNo ratings yet
- 11 9700 23 2019 165347.inddDocument2 pages11 9700 23 2019 165347.inddAya TharwatNo ratings yet
- Imaging Anatomy Brain and Spine Anne G Osborn Full ChapterDocument67 pagesImaging Anatomy Brain and Spine Anne G Osborn Full Chaptervicki.wilson456100% (8)
- Population Ecology: Aecc-I +3 1 YearDocument32 pagesPopulation Ecology: Aecc-I +3 1 YearAnita kumari SahuNo ratings yet
- ANIMILIADocument10 pagesANIMILIAAnand Teekmani AnuNo ratings yet
- Esthetic Dentistry / Orthodontic Courses by Indian Dental AcademyDocument256 pagesEsthetic Dentistry / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- His T PathologyDocument23 pagesHis T PathologygauravNo ratings yet
- Klasmann Peat Substrates Product Information - ForemostCoDocument32 pagesKlasmann Peat Substrates Product Information - ForemostCoMuhamad FajarNo ratings yet
- Allegra 64R CentrifugeDocument64 pagesAllegra 64R Centrifugeluroguita-1No ratings yet
- Erickson's Psycho-Social Theory of DevelopmentDocument29 pagesErickson's Psycho-Social Theory of Developmentexodo loverNo ratings yet
- Stress Management For TeachersDocument44 pagesStress Management For TeacherscikgulazimNo ratings yet
- Pediatric RehabDocument32 pagesPediatric RehabRainy DaysNo ratings yet
- Kombinasi Pengaruh Media Tanam Akar Pakis Dan Arang Sekam Terhadap Perkecambahan Dan Pertumbuhan Bibit EucalyptusDocument9 pagesKombinasi Pengaruh Media Tanam Akar Pakis Dan Arang Sekam Terhadap Perkecambahan Dan Pertumbuhan Bibit EucalyptusNeta AdzkiyaNo ratings yet
- CV of C.v.narasimha MurthyDocument4 pagesCV of C.v.narasimha MurthyNarasimha MurthyNo ratings yet
- Om Biomerieux Reagents Ot-43871 Package Insert-43871Document3 pagesOm Biomerieux Reagents Ot-43871 Package Insert-43871Salomon SalomonNo ratings yet
- Molecular Docking in Structure-Based Drug DesignDocument33 pagesMolecular Docking in Structure-Based Drug DesignIvan Tubert-BrohmanNo ratings yet
- TC18Document3 pagesTC18Robert BarnesNo ratings yet
- Symbiotic Relationships Chart AnswersDocument2 pagesSymbiotic Relationships Chart AnswersLiwayway Araza100% (1)
- EXPERIMENT 9 Food ChemistryDocument7 pagesEXPERIMENT 9 Food ChemistryNurmazillazainal67% (3)
- BajraDocument6 pagesBajraASHUTOSH MOHANTYNo ratings yet
- Lesson-Plan Ecologica RelationshipDocument10 pagesLesson-Plan Ecologica RelationshipRen Mart Decipeda100% (3)
- Microbiology 1.03 Basic Concepts 1Document9 pagesMicrobiology 1.03 Basic Concepts 1Camila BarzagaNo ratings yet
- Ali Raza Forensic SupplementsDocument120 pagesAli Raza Forensic Supplementsumerq604No ratings yet
- Cost-Effective Production of Arthrospira (Spirulina) PlatensisDocument6 pagesCost-Effective Production of Arthrospira (Spirulina) PlatensisRafael BendezúNo ratings yet
- A History of Membrane Transport and Bioenergetics PDFDocument383 pagesA History of Membrane Transport and Bioenergetics PDFEdmilson RodriguesNo ratings yet
- GPB 321 Crop Improvement Manual FinalDocument71 pagesGPB 321 Crop Improvement Manual FinalSultan AhmadNo ratings yet
- Anatomical Features of Bougainvillea (Nyctaginaceae) : Sarah ChewDocument7 pagesAnatomical Features of Bougainvillea (Nyctaginaceae) : Sarah ChewPratistha ShauryaNo ratings yet
- Grade8 STE Biotech Q4 Module 2 Wk3-4 ADMDocument24 pagesGrade8 STE Biotech Q4 Module 2 Wk3-4 ADMJohn Patrick Abraham91% (11)