You might also like
- CDC Internal COVID-19 Delta Variant DocumentDocument25 pagesCDC Internal COVID-19 Delta Variant DocumentAdam Forgie100% (3)
- Vaccination Records - AdultsDocument2 pagesVaccination Records - AdultsverumluxNo ratings yet
- Joyce Brennfleck Shannon - Drug Abuse Sourcebook, Third Edition (2010) PDFDocument634 pagesJoyce Brennfleck Shannon - Drug Abuse Sourcebook, Third Edition (2010) PDFMarciano EtvaldoNo ratings yet
- Overview AHM 250Document6 pagesOverview AHM 250swati_kota110% (2)
- Cancellation Form Refund RequestDocument2 pagesCancellation Form Refund RequestVinh Duong0% (1)
- Falcon SPM Paper 2Document25 pagesFalcon SPM Paper 2175 Yellamraju Vidhatri0% (1)
- PMTCT: Reducing Mother-to-Child HIV TransmissionDocument56 pagesPMTCT: Reducing Mother-to-Child HIV TransmissionCica ClarissaNo ratings yet
- Integrated Management of Childhood IllnessDocument8 pagesIntegrated Management of Childhood IllnessSehar162No ratings yet
- Challenges in VH Treatment: Fmoh 2021Document17 pagesChallenges in VH Treatment: Fmoh 2021Eleni HagosNo ratings yet
- Challenges of Achieving Viral Hepatitis Treatment Targets in EthiopiaDocument16 pagesChallenges of Achieving Viral Hepatitis Treatment Targets in EthiopiaEleni HagosNo ratings yet
- Quiz 3 MicroeconomicsDocument3 pagesQuiz 3 MicroeconomicsNguyễn Đức ThắngNo ratings yet
- xxx-ILC 4.2-024 Poster-Shahed Hossain Bangladesh-2 PDFDocument22 pagesxxx-ILC 4.2-024 Poster-Shahed Hossain Bangladesh-2 PDFRahen Rangan100% (1)
- Bishan Guracha Orientation 1Document114 pagesBishan Guracha Orientation 1nani babyNo ratings yet
- RSUD Jayapura HIV/AIDS ServicesDocument48 pagesRSUD Jayapura HIV/AIDS ServicesStevanus Bob Arvianto AlwieNo ratings yet
- Management of MRSA NP: Slide ReferenceDocument29 pagesManagement of MRSA NP: Slide ReferenceDermawan SolehNo ratings yet
- Il Documento Dei CDC Americani Sulla Variante Delta CovidDocument25 pagesIl Documento Dei CDC Americani Sulla Variante Delta CovidIda ArtiacoNo ratings yet
- CDC: Improving Communications Around Vaccine Breakthrough and Vaccine EffectivenessDocument25 pagesCDC: Improving Communications Around Vaccine Breakthrough and Vaccine EffectivenessCNBC.com100% (1)
- Review & Critical Appraisal of Newborn Health ProgramsDocument47 pagesReview & Critical Appraisal of Newborn Health ProgramsSagar ParajuliNo ratings yet
- AidsDocument28 pagesAidsTee Kok KeongNo ratings yet
- 2016 InglésDocument28 pages2016 InglésJuan Felipe RunzaNo ratings yet
- Mamas 2Document6 pagesMamas 2DIOGENESNo ratings yet
- Can We Afford Social Security and Medicare For 76 Million Boomers? (David C. John)Document14 pagesCan We Afford Social Security and Medicare For 76 Million Boomers? (David C. John)National Press FoundationNo ratings yet
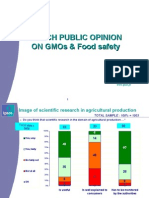
- French Public Opinion On Gmos & Food SafetyDocument12 pagesFrench Public Opinion On Gmos & Food SafetyelplastiNo ratings yet
- 2008 TMA Physician SurveyDocument21 pages2008 TMA Physician SurveySteve LevineNo ratings yet
- Dwi Handono Sulistyo KMPK Fk-UgmDocument43 pagesDwi Handono Sulistyo KMPK Fk-UgmRani Khairan Nisa'No ratings yet
- Hasil Pencapaian Indikator Mdgs Puskesmas Mamajang TAHUN 2016Document11 pagesHasil Pencapaian Indikator Mdgs Puskesmas Mamajang TAHUN 2016MuMu GuevaraNo ratings yet
- Formal Final ResutlDocument11 pagesFormal Final ResutlEngr Sardar Umer KhalidNo ratings yet
- Tuberculosis in Developing Countries: Dilemmas: Erik Post, MD MSC Royal Tropical Institute AmsterdamDocument23 pagesTuberculosis in Developing Countries: Dilemmas: Erik Post, MD MSC Royal Tropical Institute Amsterdamgaruda unriNo ratings yet
- Acne Vulgaris 1Document4 pagesAcne Vulgaris 1Ridho ForesNo ratings yet
- Direct2lab Pathology MKTDocument7 pagesDirect2lab Pathology MKTAvinash JhaNo ratings yet
- Situasi Global PD3I 7 Feb 2022Document21 pagesSituasi Global PD3I 7 Feb 2022FAIZ FANINo ratings yet
- ECHO Indicators AnalysisDocument3 pagesECHO Indicators AnalysisNgoma TélesphoreNo ratings yet
- Nay Pyi Taw Regional Public Health Department: Annual Programme Review of Newborn and Child Health DevelopmentDocument21 pagesNay Pyi Taw Regional Public Health Department: Annual Programme Review of Newborn and Child Health DevelopmentP&S NpwNo ratings yet
- Afar HIV Situation For DICDocument45 pagesAfar HIV Situation For DICUsman Kazali AbdulkadirNo ratings yet
- The in Uence of Balanced Counseling Strategy On Mother Toward Use of Post Partum Family PlanningDocument5 pagesThe in Uence of Balanced Counseling Strategy On Mother Toward Use of Post Partum Family PlanningAstri YuliandiniNo ratings yet
- National AIDS Control Programme: First Quarterly Review Meeting 19 and 20 September 2019Document31 pagesNational AIDS Control Programme: First Quarterly Review Meeting 19 and 20 September 2019chitrakshi khairnarNo ratings yet
- Overview of EPI MyanmarDocument77 pagesOverview of EPI MyanmarSoe Htike0% (1)
- SIPDocument20 pagesSIPSanket Bhondage0% (1)
- Vaccinology 2017 Suchada JiamsiriDocument19 pagesVaccinology 2017 Suchada Jiamsirimauricio ramosNo ratings yet
- Icra 10Document6 pagesIcra 10tanna dixitNo ratings yet
- Unaids Fast Track Ending Aids Epidemic 2030 ReportDocument40 pagesUnaids Fast Track Ending Aids Epidemic 2030 Reporthisaya katagamiNo ratings yet
- Cervical Cancer Idn 2021 Country Profile enDocument1 pageCervical Cancer Idn 2021 Country Profile enMargareta OktavianiNo ratings yet
- Thursday KienyDocument45 pagesThursday KienyNational Press FoundationNo ratings yet
- Annual Performance Review TemplateDocument20 pagesAnnual Performance Review TemplateFrederick AgyeiNo ratings yet
- Covid19 The Impact On Healthcare ExpenditureDocument9 pagesCovid19 The Impact On Healthcare ExpenditureDavid ChueNo ratings yet
- Adjusted Dynamics of COVID-19 Pandemic Due To Herd Immunity in BangladeshDocument16 pagesAdjusted Dynamics of COVID-19 Pandemic Due To Herd Immunity in BangladeshNazmul IslamNo ratings yet
- Trends in Telehealth: Alex Gerwer Principal Partner AKNDocument60 pagesTrends in Telehealth: Alex Gerwer Principal Partner AKNasg_akn8335No ratings yet
- Obstetrics: D.A. Mousa M.A. Mohammad A.B. ToboliDocument8 pagesObstetrics: D.A. Mousa M.A. Mohammad A.B. Toboligusti ayu azzahra Shabrina p.bNo ratings yet
- Exit Strategy of COVID-19 Epidemic in Sri LankaDocument17 pagesExit Strategy of COVID-19 Epidemic in Sri LankagazNo ratings yet
- Grand Forks Weekly COVID-19 Update April 15Document10 pagesGrand Forks Weekly COVID-19 Update April 15inforumdocsNo ratings yet
- Dr. Arto Yuwono Soeroto's Recommendations on Covid-19 VaccinationDocument35 pagesDr. Arto Yuwono Soeroto's Recommendations on Covid-19 VaccinationekaNo ratings yet
- GPH Tutok Gamutan Davao OrientalDocument3 pagesGPH Tutok Gamutan Davao Orientalrizza RiveraNo ratings yet
- September Ward AuditDocument5 pagesSeptember Ward AuditJhessie ChingNo ratings yet
- Philippine Health Agenda Reforms and AchievementsDocument45 pagesPhilippine Health Agenda Reforms and AchievementsAmil P. Tan IINo ratings yet
- VTE ProphylaxisDocument17 pagesVTE ProphylaxisPeter McManusNo ratings yet
- Review & Critical Appraisal of Newborn Health Programs - DRHNDocument44 pagesReview & Critical Appraisal of Newborn Health Programs - DRHNSagar ParajuliNo ratings yet
- POE POLIO - FinalDocument84 pagesPOE POLIO - FinalOrlando BaltodanoNo ratings yet
- CFR - Why Vaccination Coverage Is Crucial for COVID-19Document9 pagesCFR - Why Vaccination Coverage Is Crucial for COVID-19ioannis tsagarliotisNo ratings yet
- 2020 Employer Telework Survey PresentationDocument23 pages2020 Employer Telework Survey PresentationDCOH EditorNo ratings yet
- OHSU COVID Forecast: Edition: 12/17/2021Document46 pagesOHSU COVID Forecast: Edition: 12/17/2021Sinclair Broadcast Group - EugeneNo ratings yet
- Prof. Lesmana - The 4th Liv GI Fair PGC On Hepatitis C Evolution of DAA (Direct Acting Antiviral AgentDocument26 pagesProf. Lesmana - The 4th Liv GI Fair PGC On Hepatitis C Evolution of DAA (Direct Acting Antiviral AgentWenny NgawingNo ratings yet
- El Cambio Climático y La Seguridad Alimentaria 2023Document2 pagesEl Cambio Climático y La Seguridad Alimentaria 2023ramonrosalesNo ratings yet
- HIV/AIDS Management Updates in NamibiaDocument45 pagesHIV/AIDS Management Updates in NamibiaKeletso NyathiNo ratings yet
- Care For Vulnerable Populations During COVID-19 PandemicFrom EverandCare For Vulnerable Populations During COVID-19 PandemicNo ratings yet
- HEALTHCARE SERVICE QUALITY AND PATIENT SATISFACTION IN OMANI PUBLIC HOSPITALS THROUGHOUT COVID-19 ERA: AN EMPIRICAL INVESTIGATIONFrom EverandHEALTHCARE SERVICE QUALITY AND PATIENT SATISFACTION IN OMANI PUBLIC HOSPITALS THROUGHOUT COVID-19 ERA: AN EMPIRICAL INVESTIGATIONNo ratings yet
- Public Private Partnerships Booket-2018Document44 pagesPublic Private Partnerships Booket-2018Prabir Kumar ChatterjeeNo ratings yet
- Medical CorporationDocument1 pageMedical CorporationPrabir Kumar ChatterjeeNo ratings yet
- Emvolio Pilot Strategy DocumentDocument34 pagesEmvolio Pilot Strategy DocumentPrabir Kumar ChatterjeeNo ratings yet
- SCDS, Draft PolicyDocument33 pagesSCDS, Draft PolicyPrabir Kumar ChatterjeeNo ratings yet
- Sickle Cell Screening 21 March 2018Document2 pagesSickle Cell Screening 21 March 2018Prabir Kumar ChatterjeeNo ratings yet
- Final ANM Malaria Guideline-2014Document10 pagesFinal ANM Malaria Guideline-2014Prabir Kumar ChatterjeeNo ratings yet
- BNSL 043 Block 4Document140 pagesBNSL 043 Block 4Prabir Kumar Chatterjee100% (3)
- Leprosy Policy BriefDocument4 pagesLeprosy Policy BriefPrabir Kumar ChatterjeeNo ratings yet
- TB - Policy Brief v2Document4 pagesTB - Policy Brief v2Prabir Kumar ChatterjeeNo ratings yet
- OWH On CancerDocument24 pagesOWH On CancerPrabir Kumar ChatterjeeNo ratings yet
- Fulwari SpacesDocument44 pagesFulwari SpacesPrabir Kumar ChatterjeeNo ratings yet
- Operational Guidelines LMISDocument19 pagesOperational Guidelines LMISPrabir Kumar ChatterjeeNo ratings yet
- MLHP Design Issues Concept Note June 24 2018Document7 pagesMLHP Design Issues Concept Note June 24 2018Prabir Kumar Chatterjee100% (2)
- Orientation of MAS Members On JaundiceDocument2 pagesOrientation of MAS Members On JaundicePrabir Kumar ChatterjeeNo ratings yet
- How To Collect HMIS Data For BlocksDocument4 pagesHow To Collect HMIS Data For BlocksPrabir Kumar ChatterjeeNo ratings yet
- VedantaDocument1 pageVedantaPrabir Kumar ChatterjeeNo ratings yet
- SELCO Health Workshop Concept and AgendaDocument2 pagesSELCO Health Workshop Concept and AgendaPrabir Kumar ChatterjeeNo ratings yet
- Vedanta HospitalDocument1 pageVedanta HospitalPrabir Kumar ChatterjeeNo ratings yet
- NHM SpendingDocument8 pagesNHM SpendingPrabir Kumar ChatterjeeNo ratings yet
- CEEW CG HighlightsDocument4 pagesCEEW CG HighlightsPrabir Kumar ChatterjeeNo ratings yet
- Upright GMS 1977Document17 pagesUpright GMS 1977Prabir Kumar ChatterjeeNo ratings yet
- Budget For One AMRIT ClinicDocument4 pagesBudget For One AMRIT ClinicPrabir Kumar ChatterjeeNo ratings yet
- 2 Reggie Lepcha GMS 1977Document1 page2 Reggie Lepcha GMS 1977Prabir Kumar ChatterjeeNo ratings yet
- Raigarh Report PDFDocument52 pagesRaigarh Report PDFPrabir Kumar ChatterjeeNo ratings yet
- Arc GIS Make A MapDocument11 pagesArc GIS Make A MapPrabir Kumar ChatterjeeNo ratings yet
- Raigarh SummaryDocument30 pagesRaigarh SummaryPrabir Kumar ChatterjeeNo ratings yet
- Chhattisgarh Yuva015Document2 pagesChhattisgarh Yuva015Prabir Kumar ChatterjeeNo ratings yet
- Saharias and TBDocument20 pagesSaharias and TBPrabir Kumar ChatterjeeNo ratings yet
- Jip (P 3T?C - 3 Lajg: Uau Ik XK Hkiifi XytDocument1 pageJip (P 3T?C - 3 Lajg: Uau Ik XK Hkiifi XytPrabir Kumar ChatterjeeNo ratings yet
- Search of Gunda Dhur - 1910Document8 pagesSearch of Gunda Dhur - 1910Prabir Kumar ChatterjeeNo ratings yet
- Getting Early Prenatal CareDocument8 pagesGetting Early Prenatal CareChris GuisadioNo ratings yet
- GHPRDocument2 pagesGHPRGuroo NanakNo ratings yet
- CII & KPMG The Emerging Role of PPP in Indian Healthcare Sector PolicyPaper PDFDocument37 pagesCII & KPMG The Emerging Role of PPP in Indian Healthcare Sector PolicyPaper PDFAnanya DasguptaNo ratings yet
- Vaccination Schedule: Infants Toddlers Children Adolescents AdultsDocument1 pageVaccination Schedule: Infants Toddlers Children Adolescents AdultsIsais NNo ratings yet
- The Laboratory of Pharmacokinetics, Dept. of Pharmacy, University of PatrasDocument1 pageThe Laboratory of Pharmacokinetics, Dept. of Pharmacy, University of PatrasnosfarNo ratings yet
- WHO RHR 19.20 Eng PDFDocument4 pagesWHO RHR 19.20 Eng PDFElsa SembiringNo ratings yet
- The Real Facts - CV19-4Document17 pagesThe Real Facts - CV19-4Ale YankNo ratings yet
- Public Health Lab RolesDocument45 pagesPublic Health Lab RolesLarisa Izabela AndronecNo ratings yet
- Government & Non-Governmental Structures Concept MapDocument1 pageGovernment & Non-Governmental Structures Concept MapLynelle BernardoNo ratings yet
- Drug Reimbursement Regulation in 6 Peer CountriesDocument8 pagesDrug Reimbursement Regulation in 6 Peer CountriessunnyNo ratings yet
- Phil Health Quiz Bee Questions EasyDocument3 pagesPhil Health Quiz Bee Questions EasyMae Ann DaganosNo ratings yet
- Complete Children's ImmunizationDocument6 pagesComplete Children's ImmunizationAshley Castelo0% (1)
- Condom UseDocument2 pagesCondom UseMuhamad FakhrullahNo ratings yet
- Pak Ketut 1 PDFDocument32 pagesPak Ketut 1 PDFArini Aprilliani LanriNo ratings yet
- Essential Drugs at PHCDocument21 pagesEssential Drugs at PHCapi-3823785No ratings yet
- 11 4 Calibo PDFDocument34 pages11 4 Calibo PDFnelmaNo ratings yet
- The EPIDocument14 pagesThe EPIMartin Dazel Martin DazelNo ratings yet
- Midterm Review QuestionsDocument6 pagesMidterm Review QuestionsMaryam Amatullah-DanzyNo ratings yet
- Understanding Tuberculosis: Causes, Symptoms, Treatment and PreventionDocument29 pagesUnderstanding Tuberculosis: Causes, Symptoms, Treatment and PreventionRamandeep KaurNo ratings yet
- Compartmental & Non-Compartmental PharmacokineticsDocument21 pagesCompartmental & Non-Compartmental PharmacokineticsVikas JhawatNo ratings yet
- SOP Funding RequestDocument4 pagesSOP Funding RequestFitriwardahNo ratings yet
- Na PDP Classic Eoc 2022 Na2pdgeoc79428e RDocument146 pagesNa PDP Classic Eoc 2022 Na2pdgeoc79428e RMelva MosleyNo ratings yet