You might also like
- Nps Technical Rescue Handbook 2014 PDFDocument292 pagesNps Technical Rescue Handbook 2014 PDFMatheus Baños100% (1)
- D.2 - Business Continuity Plan DocumentDocument35 pagesD.2 - Business Continuity Plan DocumentNikitasKladakis100% (1)
- 1-Model Emergency Drill PlanDocument7 pages1-Model Emergency Drill PlanUdhaya KumarNo ratings yet
- Purpose: Title: Code Pink-Abduction PlanDocument5 pagesPurpose: Title: Code Pink-Abduction Planarie susantoNo ratings yet
- Fire Drill Audit ChecklistDocument5 pagesFire Drill Audit ChecklistGoh Boon TiongNo ratings yet
- Ambulance Best Practice Report EnglishDocument23 pagesAmbulance Best Practice Report EnglishYasir RazaNo ratings yet
- G.2.8 - MFD Medical Emergency Response PlanDocument29 pagesG.2.8 - MFD Medical Emergency Response Planالحاج راضي راضيNo ratings yet
- Incident Reporting and Investigation GuidanceDocument2 pagesIncident Reporting and Investigation GuidanceMuhammad SuhaibNo ratings yet
- Emergency Response Plan - SuperbsafetyengineersDocument27 pagesEmergency Response Plan - SuperbsafetyengineersPaulina PaskahriaNo ratings yet
- Hospital Emergency Management PlanDocument5 pagesHospital Emergency Management PlandedefreddyNo ratings yet
- Basic Rope Rescue Training WorkshopDocument4 pagesBasic Rope Rescue Training WorkshopMayeth Alquizalas FazonNo ratings yet
- Medical Evacuation Plan ModifiedDocument8 pagesMedical Evacuation Plan Modifieddr.rahul mathewNo ratings yet
- Toledo Code Blue PolicyDocument4 pagesToledo Code Blue PolicySt SNo ratings yet
- Incident Investigation (2020)Document77 pagesIncident Investigation (2020)Elchin100% (1)
- NDRRMC - 221Document5 pagesNDRRMC - 221Joselito Macatangay Castro100% (1)
- IMH Handbook 2021Document232 pagesIMH Handbook 2021jarmandia100% (1)
- Lifeline 16911 Ambulance Disinfection & Decontamination Cleaning Protocols 2020Document69 pagesLifeline 16911 Ambulance Disinfection & Decontamination Cleaning Protocols 2020Michael Deakin100% (1)
- 2.12 ICS Forms ICS 202Document2 pages2.12 ICS Forms ICS 202mdrrmo sinait100% (1)
- Mass Casualty Emergency Plan: An Overview ofDocument13 pagesMass Casualty Emergency Plan: An Overview ofBishnu Prasad JenaNo ratings yet
- Medical Services and ManagementDocument17 pagesMedical Services and ManagementjohnNo ratings yet
- Incident Reporting PolicyDocument5 pagesIncident Reporting Policyemeka2012No ratings yet
- JCI QUESTIONNAIRE-PCI Dept.Document6 pagesJCI QUESTIONNAIRE-PCI Dept.Rabiya Sajjad100% (2)
- Incident Command SystemDocument29 pagesIncident Command SystemFrank Sumalpong100% (6)
- Emergency Planning FinalDocument31 pagesEmergency Planning Finalالحاج راضي راضيNo ratings yet
- Proposed COVID-19 Response PlanDocument12 pagesProposed COVID-19 Response PlanRabindra Raj PantaNo ratings yet
- Autoclave GuideDocument48 pagesAutoclave GuideIman 111No ratings yet
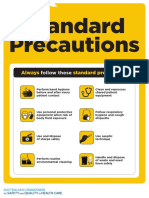
- Approach 4 Standard Precautions Icon PDF 672KBDocument1 pageApproach 4 Standard Precautions Icon PDF 672KBElaine MacalandaNo ratings yet
- Module 5 - Incident Event Assessment and Management by Objectives 3Document45 pagesModule 5 - Incident Event Assessment and Management by Objectives 3fernando jose DancilNo ratings yet
- Emergency Evacuation PlanDocument14 pagesEmergency Evacuation PlanGlenn MadeloNo ratings yet
- Fire Safety OfficerDocument2 pagesFire Safety OfficerMurali ManoharNo ratings yet
- Radiology ServicesDocument5 pagesRadiology Servicesshah007zaadNo ratings yet
- Emergency CodesDocument23 pagesEmergency CodesJennifer B. GarciaNo ratings yet
- Mock Drill Manual On DisastersDocument22 pagesMock Drill Manual On DisastersshrutikesavanNo ratings yet
- Hospital EvacuationDocument19 pagesHospital EvacuationShiladitya ChatterjeeNo ratings yet
- 3a - Occupational Safety ME 70 Basic Occupational Safety and HealthDocument91 pages3a - Occupational Safety ME 70 Basic Occupational Safety and Healths.salise.allendaveNo ratings yet
- How To Identify and Analyze A Hospital Risk Assessment: Risk Management Part of The Higher PlanDocument12 pagesHow To Identify and Analyze A Hospital Risk Assessment: Risk Management Part of The Higher Planver_at_workNo ratings yet
- IMPLAN SAKLOLO On Policing During Disaster PPTX AutosavedDocument75 pagesIMPLAN SAKLOLO On Policing During Disaster PPTX AutosavedMelba90% (10)
- Hospital Safety PromotionDocument46 pagesHospital Safety PromotionRhodora BenipayoNo ratings yet
- AZSPU Legionella Control Management ProgrammeDocument38 pagesAZSPU Legionella Control Management ProgrammeAmir M. ShaikhNo ratings yet
- Disaster Management Plan For Hospitals: Hospital OperationsDocument59 pagesDisaster Management Plan For Hospitals: Hospital OperationsGaurav BhawsarNo ratings yet
- AZSPU Lesson Learned Communication ProcessDocument17 pagesAZSPU Lesson Learned Communication ProcessAmir M. ShaikhNo ratings yet
- Hospital Disaster Management Plan - Draft1-MkDocument71 pagesHospital Disaster Management Plan - Draft1-MkAdri FitriNo ratings yet
- Code Blue System: Hospital Sultanah Aminah Johor BahruDocument15 pagesCode Blue System: Hospital Sultanah Aminah Johor BahrumursidahanimNo ratings yet
- Hospital Emergency & Evacuation ProcedureDocument4 pagesHospital Emergency & Evacuation ProcedureIka LiaNo ratings yet
- Identifying and Controlling Hazards: We Lco MeDocument45 pagesIdentifying and Controlling Hazards: We Lco MeAijaz Ahmed ShaikhNo ratings yet
- Annual Infection Control Report Für 2021Document26 pagesAnnual Infection Control Report Für 2021Ruby Joyce AguilarNo ratings yet
- Hurricane Harvery AAR - FinalDocument64 pagesHurricane Harvery AAR - FinalepraetorianNo ratings yet
- Clinical Casuality ManagementDocument6 pagesClinical Casuality ManagementswathiprasadNo ratings yet
- BFD SOP 10 Fires in TaxpayersDocument12 pagesBFD SOP 10 Fires in TaxpayersPEDRO CAPARACHIN PALPANo ratings yet
- FEMA Emergency Response Plan 0Document10 pagesFEMA Emergency Response Plan 0Adam WardNo ratings yet
- 1.1 Hospital Fire PlanDocument8 pages1.1 Hospital Fire Planjcspai100% (2)
- NDRP Consequence Management For Terrorism Related IncidentsDocument134 pagesNDRP Consequence Management For Terrorism Related IncidentsMahar LagmayNo ratings yet
- prehospital-EMS-COVID-19-recommendations - 4.4Document19 pagesprehospital-EMS-COVID-19-recommendations - 4.4MEONENo ratings yet
- CHA Hospital Activation of The Emergency Operations Plan ChecklistDocument5 pagesCHA Hospital Activation of The Emergency Operations Plan Checklistraysub159No ratings yet
- Interfacility Referral Protocol Revised May 2017Document7 pagesInterfacility Referral Protocol Revised May 2017meljamerlanNo ratings yet
- MDPH Hospital Based Decontamination Resources June 2014Document122 pagesMDPH Hospital Based Decontamination Resources June 2014jwmeadow2401No ratings yet
- 5 (A) Safe Use and Disposal of Sharps: Review Date: April 2010Document4 pages5 (A) Safe Use and Disposal of Sharps: Review Date: April 2010megha_gNo ratings yet
- Health & Safety, Covid-19 Safety Protocols To Be Adopted For Construction of The Wesley/Conference Office Building Project, Ridge-AccraDocument22 pagesHealth & Safety, Covid-19 Safety Protocols To Be Adopted For Construction of The Wesley/Conference Office Building Project, Ridge-Accraemmanuel SiawNo ratings yet
- (Facility Name) : Emergency Operations PlanDocument26 pages(Facility Name) : Emergency Operations PlanIbsen CampoverdeNo ratings yet
- First Aid Plan ConstructionDocument13 pagesFirst Aid Plan ConstructionUmair KhanNo ratings yet
- NFPA Label and GHS PictogramsDocument2 pagesNFPA Label and GHS PictogramsPrakharNo ratings yet
- Bloodborne and Airborne Pathogens: (Universal Precautions)Document2 pagesBloodborne and Airborne Pathogens: (Universal Precautions)roberto_00643557No ratings yet
- HSSE Statistics For The Past 5 YearsDocument4 pagesHSSE Statistics For The Past 5 YearsNikhil VermaNo ratings yet
- Health and Safety Risk Assessment: Activity Hazard Risk Rating (0 Low, 5 High) SolutionDocument2 pagesHealth and Safety Risk Assessment: Activity Hazard Risk Rating (0 Low, 5 High) SolutionBarry TuriNo ratings yet
- Hrva ToolsDocument59 pagesHrva Toolsretno wahyuNo ratings yet
- Standardized Hospital Colour CodesDocument5 pagesStandardized Hospital Colour CodesRichard Deo R. AlaveNo ratings yet
- Proposal For ImprovementDocument22 pagesProposal For ImprovementJohn Ervin AgenaNo ratings yet
- Clinical Practice in AmbulanceDocument4 pagesClinical Practice in Ambulancengurah_wardanaNo ratings yet
- DSE Workstation Checklist Mar 2006Document9 pagesDSE Workstation Checklist Mar 2006shaistaNo ratings yet
- SOP 8, 20: OT and CSSD: 1. PurposeDocument9 pagesSOP 8, 20: OT and CSSD: 1. Purposeshah007zaadNo ratings yet
- DPP-CFT-003 Chemical Spill Control &spill KitsDocument5 pagesDPP-CFT-003 Chemical Spill Control &spill Kitsn76961No ratings yet
- TESDADocument20 pagesTESDAKissy BesarioNo ratings yet
- Airport Firefighter: Tandard ASKDocument19 pagesAirport Firefighter: Tandard ASKFranciscoVicenteNo ratings yet
- Medical Surgical Nursing Practice Exam X 50 ItemsDocument15 pagesMedical Surgical Nursing Practice Exam X 50 ItemsclobregasNo ratings yet
- MEMS Student Manual 2013aDocument16 pagesMEMS Student Manual 2013adaridlaaNo ratings yet
- Ics Form 214Document3 pagesIcs Form 214Ferdinand M. TurbanosNo ratings yet
- Standard Operating Procedures Manual: Monterey County Sheriff'S Advisory Council Search and Rescue TeamDocument24 pagesStandard Operating Procedures Manual: Monterey County Sheriff'S Advisory Council Search and Rescue TeamDan ColniceanuNo ratings yet
- Massive Leak of Liquefied Chlorine GasDocument31 pagesMassive Leak of Liquefied Chlorine GasAbdullahNo ratings yet
- Family Reunification Plan Version 2Document31 pagesFamily Reunification Plan Version 2gusyahri001No ratings yet
- Joint Mou Polk Cty HospDocument4 pagesJoint Mou Polk Cty HospJenalyn VargasNo ratings yet
- Samantha Serpas ResumeDocument1 pageSamantha Serpas Resumeapi-247085580No ratings yet
- Disaster Recovery Manager Consultant in Washington DC Resume Edwin Kenneth BarksdaleDocument3 pagesDisaster Recovery Manager Consultant in Washington DC Resume Edwin Kenneth BarksdaleEKennethBarksdaleNo ratings yet
- Rescue Response Gear Rigging Lab Sisters, OR Rope Rescue Course TextDocument32 pagesRescue Response Gear Rigging Lab Sisters, OR Rope Rescue Course TextИлья НикульшинNo ratings yet
- CDF Training and Academy Course Catalog: State of California Department of Forestry and Fire ProtectionDocument61 pagesCDF Training and Academy Course Catalog: State of California Department of Forestry and Fire ProtectionFG SummerNo ratings yet
- Crisis Management: Marilyn P. FlorendoDocument7 pagesCrisis Management: Marilyn P. FlorendoJonalyn C Piasan-NgappolNo ratings yet
- Pediatric Disaster PreparednessDocument196 pagesPediatric Disaster Preparednessccbrown7100% (1)
- Post-Activity Report Eoc TrainingDocument25 pagesPost-Activity Report Eoc TrainingKATHLEEN PONCE COCHARONo ratings yet
- Commodity Preparedness and Incident Management Reference SheetDocument17 pagesCommodity Preparedness and Incident Management Reference Sheetjulianopetry10No ratings yet
- FireDocument4 pagesFireChristopher PjunatasNo ratings yet