You might also like
- Psychiatric Nursing Care PlansDocument118 pagesPsychiatric Nursing Care PlansUrlam Kumar100% (4)
- Case Study SchizophreniaDocument3 pagesCase Study SchizophreniaCHRISANTO ARZANANNo ratings yet
- Gordons Threatened AbortionDocument2 pagesGordons Threatened AbortionRobel_Saoi_2309No ratings yet
- Schizophrenia Care Plan RNDocument8 pagesSchizophrenia Care Plan RNlisa75% (4)
- Nursing Care Plan (Bell's Palsy)Document3 pagesNursing Care Plan (Bell's Palsy)Yessamin Paith Roderos100% (3)
- Dementia Nursing Care PlanDocument2 pagesDementia Nursing Care Planmp175767% (3)
- Panic Attack Nursing Care PlanDocument4 pagesPanic Attack Nursing Care PlanSamVelasco100% (2)
- InterviewDocument5 pagesInterviewGracie S. VergaraNo ratings yet
- Risk For ViolenceDocument5 pagesRisk For Violencemikaela_pascuaNo ratings yet
- Additional Nursing Care Plans - SchizophreniaDocument26 pagesAdditional Nursing Care Plans - SchizophreniaJasmin Jacob100% (5)
- Psychiatric Nursing Care Plan For Schizoaffective DisorderDocument2 pagesPsychiatric Nursing Care Plan For Schizoaffective DisorderChelsea Williams100% (1)
- Delusional DisorderDocument12 pagesDelusional Disorderapi-3797941100% (2)
- NCP PsychosisDocument3 pagesNCP PsychosisKristian Karl Bautista Kiw-is100% (1)
- Lifestyle-Medicine Boost-Immunity FlyerDocument2 pagesLifestyle-Medicine Boost-Immunity FlyerArie AnggaNo ratings yet
- Schizophrenia NCPDocument2 pagesSchizophrenia NCPNicole cuencos100% (2)
- Anxiety Related To Stress HspitaiztionDocument1 pageAnxiety Related To Stress HspitaiztionEunice Lan Sandoval Ardiente100% (3)
- Gordon's 11 Functional Health AssessmentDocument4 pagesGordon's 11 Functional Health AssessmentJehn Pauleen Fernandez RollanNo ratings yet
- Nursing Care Plan For "Eating Disorders - Obesity"Document9 pagesNursing Care Plan For "Eating Disorders - Obesity"jhonroks100% (3)
- Nursing Care Plan For Situational Low SelfDocument5 pagesNursing Care Plan For Situational Low SelfChar Perea100% (1)
- Module 4 Standards of Psychiatric-Mental Health Nursing PracticeDocument9 pagesModule 4 Standards of Psychiatric-Mental Health Nursing Practicejoyrena ochondraNo ratings yet
- NCP Disturbed Thought Process Related To SchizophreniaDocument6 pagesNCP Disturbed Thought Process Related To Schizophrenianaishel0% (1)
- NCPDocument2 pagesNCPJoshua DecenaNo ratings yet
- The Works of Samuel Johnson, Volume 04 The Adventurer The Idler by Johnson, Samuel, 1709-1784Document297 pagesThe Works of Samuel Johnson, Volume 04 The Adventurer The Idler by Johnson, Samuel, 1709-1784Gutenberg.orgNo ratings yet
- Human Factors Classification CertificationDocument12 pagesHuman Factors Classification CertificationVinod DsouzaNo ratings yet
- NCP - BipolarDocument2 pagesNCP - BipolarSasha FongNo ratings yet
- Scizophrenia NCP2Document12 pagesScizophrenia NCP2Kholid Abu Mohammad AlfaizinNo ratings yet
- SampleStudent 3 N201ProcessRecordingDocument6 pagesSampleStudent 3 N201ProcessRecordingGracie S. Vergara100% (1)
- Care Plan 27Document10 pagesCare Plan 27Oroma TobiasNo ratings yet
- Process Recording Bipolar DisorderDocument8 pagesProcess Recording Bipolar Disorderalbert lopez100% (1)
- Defensive Coping Related To Perceived Lack of Self-Efficacy As Evidenced by Denial of Obvious ProblemsDocument2 pagesDefensive Coping Related To Perceived Lack of Self-Efficacy As Evidenced by Denial of Obvious ProblemsJeyser T. GamutiaNo ratings yet
- Schizphrenia Nursing Car PlanDocument2 pagesSchizphrenia Nursing Car PlanAmjad AliNo ratings yet
- Psych NCPDocument5 pagesPsych NCPJannen Casas100% (3)
- Submitted By: Charisa S. Simbajon BSN IvDocument8 pagesSubmitted By: Charisa S. Simbajon BSN IvCharisa Simbajon100% (1)
- NCP CamsDocument3 pagesNCP CamsNica Cielo B. LibunaoNo ratings yet
- Managing Adult Insomnia ConfidentlyDocument8 pagesManaging Adult Insomnia ConfidentlyJuliana RodriguezNo ratings yet
- NCPDocument3 pagesNCPCharles Mallari Valdez100% (1)
- Severe Anxiety As Evidenced by Repetitive ActionDocument1 pageSevere Anxiety As Evidenced by Repetitive ActionRomzy Basañes100% (3)
- Nursing CARE PLAN PsychDocument7 pagesNursing CARE PLAN Psychtiptopyo100% (1)
- Disturbed Thought Process NCP Gallano May 22 2018Document3 pagesDisturbed Thought Process NCP Gallano May 22 2018Charles Mallari ValdezNo ratings yet
- Nursing Care Plan For DepressionDocument7 pagesNursing Care Plan For DepressionCatherineNo ratings yet
- Care Plan For SchizophreniaDocument6 pagesCare Plan For SchizophreniaAllea Likestolaugh Brown100% (2)
- My Techniques For Passing SOA FSA ExamsDocument9 pagesMy Techniques For Passing SOA FSA ExamsJosh KhewNo ratings yet
- Principles of Psychiatric NursingDocument27 pagesPrinciples of Psychiatric NursingRakesh KumarNo ratings yet
- Disturbed Thought ProcessDocument4 pagesDisturbed Thought ProcessJessieRamosAnicetoNo ratings yet
- OCD NCPDocument2 pagesOCD NCPkharla suriaga100% (1)
- Actual Others-Directed Violence NCPDocument4 pagesActual Others-Directed Violence NCPNikki Ricafrente0% (2)
- Crisis Intervention: Psychiatric Nursing Nursing Care PlanDocument13 pagesCrisis Intervention: Psychiatric Nursing Nursing Care PlanKatherine 'Chingboo' Leonico Laud100% (4)
- Nursing Care Plans For Delusional DisorderDocument4 pagesNursing Care Plans For Delusional Disorderkirill61195% (22)
- NCP BSN 3rd Yr Psychiatric WardDocument9 pagesNCP BSN 3rd Yr Psychiatric WardMary Margarett BoadoNo ratings yet
- Nursing Care Plan Compromised Family CopingDocument25 pagesNursing Care Plan Compromised Family CopingNova SafitriNo ratings yet
- Example of Nursing Care Plan: Dr. Evelyn M Del MundoDocument20 pagesExample of Nursing Care Plan: Dr. Evelyn M Del MundoteuuuuNo ratings yet
- Psych NCPDocument1 pagePsych NCPEliza Joy Franco RNNo ratings yet
- NCP - Major Depressive DisorderDocument7 pagesNCP - Major Depressive DisorderJaylord Verazon100% (1)
- Disturbed Thought Processes DescribeDocument2 pagesDisturbed Thought Processes DescribePRINCESS LARA CASILAONo ratings yet
- Schizophrenia Nursing ManagementDocument56 pagesSchizophrenia Nursing ManagementHumphreyNo ratings yet
- Care PlanDocument7 pagesCare PlannasimhsNo ratings yet
- NCP FormatDocument3 pagesNCP FormatAl Bhert Timbal MagbalotNo ratings yet
- Anxiety Related To Hospitalization and Disease Condition As Manifested by Fiscal Expression and VerbalizationDocument2 pagesAnxiety Related To Hospitalization and Disease Condition As Manifested by Fiscal Expression and VerbalizationmonaNo ratings yet
- Nursing Care Plan ADocument6 pagesNursing Care Plan ACrystal WyattNo ratings yet
- Alcoholism Care PlanDocument11 pagesAlcoholism Care Planilakkiya ilakkiyaNo ratings yet
- Bipolar NCPDocument2 pagesBipolar NCPJermaine Anne MadayagNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanNeza AgdalesNo ratings yet
- Obsessive Compulsive Disorder Nursing Care Plan - Severe AnxietyDocument2 pagesObsessive Compulsive Disorder Nursing Care Plan - Severe AnxietyRnspeakcom80% (5)
- DocumentDocument10 pagesDocumentNylia AtibiNo ratings yet
- Bipolar Disorder ReportDocument6 pagesBipolar Disorder ReportLecah DevarasNo ratings yet
- SchizophreniaDocument3 pagesSchizophreniaPete Cobra Cobraiti100% (2)
- Bipolar DisordersDocument19 pagesBipolar Disordersapi-3797941No ratings yet
- Risk For Injury:: Nursing Interventions RationaleDocument14 pagesRisk For Injury:: Nursing Interventions RationalejuhlynNo ratings yet
- Toxic Relationship: Practical Steps to Quit an Abusive Relationship (Become Self-Aware Quit Manipulative and Narcissistic Behaviors to Boost Confidence)From EverandToxic Relationship: Practical Steps to Quit an Abusive Relationship (Become Self-Aware Quit Manipulative and Narcissistic Behaviors to Boost Confidence)No ratings yet
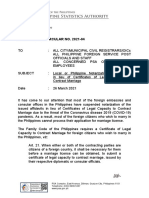
- MC NO. 2021-04 Local or Philippine Notarization of Affidavits in Lieu of Certificates of Legal Capacity To Contract MarriagesDocument4 pagesMC NO. 2021-04 Local or Philippine Notarization of Affidavits in Lieu of Certificates of Legal Capacity To Contract MarriagesGracie S. Vergara100% (1)
- Photo Composition TemplateDocument2 pagesPhoto Composition TemplateGracie S. VergaraNo ratings yet
- Cpc-Info May 23, 2023Document3 pagesCpc-Info May 23, 2023Gracie S. VergaraNo ratings yet
- Letter of IntentDocument1 pageLetter of IntentGracie S. VergaraNo ratings yet
- SupervisionDocument1 pageSupervisionGracie S. VergaraNo ratings yet
- PLANNING and EVALUATION 220117Document13 pagesPLANNING and EVALUATION 220117plethoraldorkNo ratings yet
- Possible Topics That Will Come Out (CBT Exam)Document1 pagePossible Topics That Will Come Out (CBT Exam)Gracie S. VergaraNo ratings yet
- Work (End of Shift) : Prep Kid To School Prep Kid To SchoolDocument23 pagesWork (End of Shift) : Prep Kid To School Prep Kid To SchoolGracie S. VergaraNo ratings yet
- Assessment Final ArticleDocument10 pagesAssessment Final ArticleGracie S. VergaraNo ratings yet
- JenniaDocument3 pagesJenniaGracie S. VergaraNo ratings yet
- Study GuideDocument2 pagesStudy GuideGracie S. VergaraNo ratings yet
- Drug StudyDocument6 pagesDrug StudyGracie S. VergaraNo ratings yet
- Closed Office Access Exception Request Procedure.v2Document3 pagesClosed Office Access Exception Request Procedure.v2Gracie S. VergaraNo ratings yet
- Study Guide For CBTDocument2 pagesStudy Guide For CBTGracie S. VergaraNo ratings yet
- 04 Chapter 3Document27 pages04 Chapter 3nisay_life2255100% (1)
- Additional Pointers For CBTDocument2 pagesAdditional Pointers For CBTGracie S. VergaraNo ratings yet
- Additional Pointers For CBTDocument2 pagesAdditional Pointers For CBTGracie S. VergaraNo ratings yet
- 4 Lash OriginalDocument11 pages4 Lash OriginalGracie S. VergaraNo ratings yet
- Introduction RevisionDocument50 pagesIntroduction RevisionGracie S. VergaraNo ratings yet
- Possible Topics That Will Come Out (CBT Exam)Document1 pagePossible Topics That Will Come Out (CBT Exam)Gracie S. VergaraNo ratings yet
- Application of The Modeling Role-Modeling Theory PDFDocument69 pagesApplication of The Modeling Role-Modeling Theory PDFGracie S. VergaraNo ratings yet
- ApamDocument10 pagesApamGracie S. VergaraNo ratings yet
- Possible Topics in CBTDocument2 pagesPossible Topics in CBTGracie S. VergaraNo ratings yet
- The Format: Case Study FormDocument17 pagesThe Format: Case Study FormJane DyNo ratings yet
- Modeling and Role Modeling TheoryDocument7 pagesModeling and Role Modeling TheoryGracie S. Vergara100% (1)
- The Format: Case Study FormDocument17 pagesThe Format: Case Study FormJane DyNo ratings yet
- Gordon'sDocument3 pagesGordon'sGracie S. VergaraNo ratings yet
- P.E 1 - Module - First Quarter - Health Behavior and Risk FactorsDocument30 pagesP.E 1 - Module - First Quarter - Health Behavior and Risk Factorsjohn charles garaldeNo ratings yet
- Vampire Quick Reference SheetDocument4 pagesVampire Quick Reference SheetJ&DscribdaccNo ratings yet
- Physical ExaminationDocument39 pagesPhysical ExaminationprashanthNo ratings yet
- The Vedantic Tradition in Sri Ramana MaharshiDocument24 pagesThe Vedantic Tradition in Sri Ramana MaharshiSivason100% (2)
- 1513-Article Text-6952-1-10-20200430Document7 pages1513-Article Text-6952-1-10-20200430SEAN KENZO SULITNo ratings yet
- 8 Reasons Why Rich People Hate Their Lives - 4c94778b1e0c4Document31 pages8 Reasons Why Rich People Hate Their Lives - 4c94778b1e0c4Ernani Fagundes RodriguesNo ratings yet
- The Live Lighter Handbook Stress Relief - LEVIUMDocument7 pagesThe Live Lighter Handbook Stress Relief - LEVIUMGeorgeNo ratings yet
- Sleep Quality and Stress: A Literature Review.: June 2015Document10 pagesSleep Quality and Stress: A Literature Review.: June 2015Mia Kichelle OliverosNo ratings yet
- Milestone MomentsDocument60 pagesMilestone MomentsFiorellaBeatrizNo ratings yet
- Sadeh - 2015 - Sleep AssessmentDocument16 pagesSadeh - 2015 - Sleep Assessmentguidance mtisiNo ratings yet
- Understanding How Discrimination Can Affect HealthDocument15 pagesUnderstanding How Discrimination Can Affect HealthNna HsnNo ratings yet
- Snoreben - Anti Snoring DeviceDocument14 pagesSnoreben - Anti Snoring DevicerepharmhealthcareNo ratings yet
- Bahsa InggrisDocument10 pagesBahsa InggrisDarmawan PoetraNo ratings yet
- The Concept of Qailulah (Midday Napping) From Neuroscientific and Islamic PerspectivesDocument16 pagesThe Concept of Qailulah (Midday Napping) From Neuroscientific and Islamic Perspectivesryan smithNo ratings yet
- Makalah Inggris Analytical and Hortatory ExpositionDocument7 pagesMakalah Inggris Analytical and Hortatory ExpositionIip Siti NafisahNo ratings yet
- Cause and Effect of Game Online AddictionDocument4 pagesCause and Effect of Game Online AddictionEva NurshihhahNo ratings yet
- Exam 1 May 10Document22 pagesExam 1 May 10ScribdTranslationsNo ratings yet
- Current Role of Melatonin in Pediatric Neurology: Clinical RecommendationsDocument12 pagesCurrent Role of Melatonin in Pediatric Neurology: Clinical Recommendationsdiana ndaruNo ratings yet
- Mu 75 PDFDocument4 pagesMu 75 PDFJerichoNo ratings yet
- The Elephant On Karlův Bridge Thomas TrofimukDocument303 pagesThe Elephant On Karlův Bridge Thomas TrofimukToan TranNo ratings yet
- Sleep NewletterDocument7 pagesSleep Newletterapi-270796252No ratings yet
- Critical Book Report Academic Reading Academic Written Language SkillsDocument28 pagesCritical Book Report Academic Reading Academic Written Language SkillsAzzahra Wafiq AzizaNo ratings yet
- Sleep Smarter: Bonus Resource GuideDocument7 pagesSleep Smarter: Bonus Resource GuideLaura-Georgiana MalaiasiNo ratings yet