You might also like
- LSD OD 1975 - Klock - 3266 - 1Document13 pagesLSD OD 1975 - Klock - 3266 - 10j1u9nmkv534vw9vNo ratings yet
- Coma, Hyperthermia and Bleeding Associated With Massive LSD OverdoseDocument6 pagesComa, Hyperthermia and Bleeding Associated With Massive LSD Overdose0j1u9nmkv534vw9vNo ratings yet
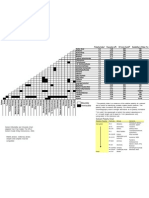
- Solvent Miscibility and Polarity ChartDocument1 pageSolvent Miscibility and Polarity Chartdiptafara100% (3)
- King Scientific CatalogueDocument694 pagesKing Scientific Catalogue0j1u9nmkv534vw9v100% (1)
- Pressure Conversion TableDocument1 pagePressure Conversion Table0j1u9nmkv534vw9vNo ratings yet
- Synthesis of Amides of Lysergic AcidDocument5 pagesSynthesis of Amides of Lysergic Acid0j1u9nmkv534vw9v100% (1)
- LSD and Its Lysergamide CousinsDocument8 pagesLSD and Its Lysergamide Cousins0j1u9nmkv534vw9vNo ratings yet
- UK Government Drug Precursors Wallchart Update February 2012Document2 pagesUK Government Drug Precursors Wallchart Update February 20120j1u9nmkv534vw9vNo ratings yet
- The Characterization of 2 - (3-Methoxyphenyl) - 2 - (Ethylamino) Cyclohexanone (Methoxetamine)Document15 pagesThe Characterization of 2 - (3-Methoxyphenyl) - 2 - (Ethylamino) Cyclohexanone (Methoxetamine)0j1u9nmkv534vw9vNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Differential Diagnosis of Complex Liver Cysts.: Poster No.: Congress: Type: AuthorsDocument20 pagesDifferential Diagnosis of Complex Liver Cysts.: Poster No.: Congress: Type: Authorsrmo.rsusNo ratings yet
- Cdem 17march WebDocument24 pagesCdem 17march WebRicardo Jonathan Ayala GarciaNo ratings yet
- Gynecology Case HistoryDocument12 pagesGynecology Case HistorySomNo ratings yet
- Apnea Del Prematuro, Practicas Actuales y Tendencias FuturasDocument14 pagesApnea Del Prematuro, Practicas Actuales y Tendencias FuturasHUMBERTO MARTiNEZ GARCiANo ratings yet
- PBL Rickets Student GuideDocument4 pagesPBL Rickets Student GuideAhmed MostafaNo ratings yet
- Putoolssect7 PDFDocument63 pagesPutoolssect7 PDFRinaNo ratings yet
- Manual of Common Bedside Surgical Procedure CHAPTER 5 - Gastrointestinal ProceduresDocument40 pagesManual of Common Bedside Surgical Procedure CHAPTER 5 - Gastrointestinal ProceduresCosti TanaseNo ratings yet
- Theroleofpain Classificationsystemsin Painmanagement: Patty Montgomery Orr,, Bettina Cobb Shank,, Amy Conner BlackDocument12 pagesTheroleofpain Classificationsystemsin Painmanagement: Patty Montgomery Orr,, Bettina Cobb Shank,, Amy Conner Blackneurologi standart4No ratings yet
- Case in Herniorraphy BESTCASEDocument23 pagesCase in Herniorraphy BESTCASEAdrian MallarNo ratings yet
- Past Psychiatric History ExamplesDocument11 pagesPast Psychiatric History ExamplesEzra Denise Lubong RamelNo ratings yet
- ACR Sample OntarioDocument5 pagesACR Sample OntarioAlisha PowerNo ratings yet
- CCRT WitzekDocument15 pagesCCRT WitzekMario Antonio FloresNo ratings yet
- Proximexa Suspension and Tablets GDS Version 25Document18 pagesProximexa Suspension and Tablets GDS Version 25Masud l NazmulNo ratings yet
- Lab FindingsDocument3 pagesLab FindingsRonica GonzagaNo ratings yet
- OSCE: Respiratory History and ExaminationDocument10 pagesOSCE: Respiratory History and ExaminationShahin KazemzadehNo ratings yet
- Essay About Why We Need Physiology in Our LifeDocument8 pagesEssay About Why We Need Physiology in Our LifeWendelieDescartinNo ratings yet
- Pathophysiology of Congestive Heart FailureDocument3 pagesPathophysiology of Congestive Heart Failuretinayko100% (1)
- Pedia QDocument36 pagesPedia QAmal100% (1)
- Acoustic NeuromaDocument14 pagesAcoustic NeuromaNeshanth SurendranNo ratings yet
- CME PRETERM LABOR, PROM, PPROM FDocument39 pagesCME PRETERM LABOR, PROM, PPROM FRatna Setia WatiNo ratings yet
- Post-Operative Fever EditDocument52 pagesPost-Operative Fever EditDebsNo ratings yet
- Communicable Disease Nursing Part II Diseases (1) 2Document21 pagesCommunicable Disease Nursing Part II Diseases (1) 2MK LiNo ratings yet
- KLSC BDU Kuwait Healthcare Report 2019 VF PDFDocument16 pagesKLSC BDU Kuwait Healthcare Report 2019 VF PDFJim MacaoNo ratings yet
- Clinical Toxicology-Poisoned Patient Cases W Answers/ExplanationsDocument7 pagesClinical Toxicology-Poisoned Patient Cases W Answers/ExplanationsMarc Imhotep Cray, M.D.100% (3)
- Evaluation of The R One Robotic System For Percutaneous Coronary Intervention THDocument11 pagesEvaluation of The R One Robotic System For Percutaneous Coronary Intervention THNeranga SamaratungeNo ratings yet
- Ma Cristy L. Exconde, MD, FPOGSDocument62 pagesMa Cristy L. Exconde, MD, FPOGSCAROL ANN PATITICO100% (1)
- Dengue Fever Treatment With Carica Papaya Leaves Extracts PDFDocument4 pagesDengue Fever Treatment With Carica Papaya Leaves Extracts PDFJulián SánchezNo ratings yet
- Comparative Evaluation of Pharmacist-Managed Vancomycin Dosing in A Community Hospital Following Implementation of A System-Wide Vancomycin Dosing GuidelineDocument9 pagesComparative Evaluation of Pharmacist-Managed Vancomycin Dosing in A Community Hospital Following Implementation of A System-Wide Vancomycin Dosing GuidelineSabrina JonesNo ratings yet
- Penatalaksanaan DemamDocument39 pagesPenatalaksanaan DemamClaraRotendownNo ratings yet
- 7 Drug CategoriesDocument2 pages7 Drug CategoriesMarian CamosaNo ratings yet