You might also like
- Lower Extremity Arterial Protocol 14 1Document2 pagesLower Extremity Arterial Protocol 14 1api-3494022400% (1)
- Mesenteric Doppler Protocol 14Document2 pagesMesenteric Doppler Protocol 14api-349402240No ratings yet
- Renal Doppler Protocol 14 1Document4 pagesRenal Doppler Protocol 14 1api-349402240100% (1)
- Upper Extremity Venous Protocol 14Document2 pagesUpper Extremity Venous Protocol 14api-349402240No ratings yet
- Lower Extremity Venous Incompetence Protcol 14Document5 pagesLower Extremity Venous Incompetence Protcol 14api-349402240No ratings yet
- Lower Extremity Arterial Protocol 14 PDFDocument2 pagesLower Extremity Arterial Protocol 14 PDFapi-390240132No ratings yet
- Upper Extremity Arterial Protocol 14 PDFDocument2 pagesUpper Extremity Arterial Protocol 14 PDFapi-390240132No ratings yet
- Study of Pediatric Congenital Cardiac Malformations by EchocardiographyDocument23 pagesStudy of Pediatric Congenital Cardiac Malformations by EchocardiographyRana Abd AlmugeethNo ratings yet
- Carotid Protocol 14 1Document4 pagesCarotid Protocol 14 1api-349402240No ratings yet
- Doppler Echocardiography: Dr.S.R.Sruthi Meenaxshi MBBS, MD, PDFDocument38 pagesDoppler Echocardiography: Dr.S.R.Sruthi Meenaxshi MBBS, MD, PDFsruthimeena6891No ratings yet
- Doppler Ultrasound of The KidneysDocument23 pagesDoppler Ultrasound of The KidneysivoklarinNo ratings yet
- Renal Artery Doppler NsDocument15 pagesRenal Artery Doppler Nss0800841739No ratings yet
- Liver Protocol 14 1Document5 pagesLiver Protocol 14 1api-349402240No ratings yet
- Appendix Protocol 14 1Document2 pagesAppendix Protocol 14 1api-349402240No ratings yet
- Us Abdominal AortaDocument16 pagesUs Abdominal AortaRomaNo ratings yet
- 5 Min - Myocardial Strain AnalysisDocument26 pages5 Min - Myocardial Strain AnalysisAsim Kumar Biswas100% (1)
- Allen Test Protocol 14 1Document2 pagesAllen Test Protocol 14 1api-349402240No ratings yet
- RV Dysfunction - Assessment by EchocardiographyDocument52 pagesRV Dysfunction - Assessment by EchocardiographyNag Mallesh RaoNo ratings yet
- Fetal Echocardiogram ProtocolDocument4 pagesFetal Echocardiogram Protocolapi-349402240No ratings yet
- Scrotum Protocol 14Document2 pagesScrotum Protocol 14api-349402240No ratings yet
- Lower Extremity Venous Protocol 14Document3 pagesLower Extremity Venous Protocol 14api-276847924No ratings yet
- Medical Ultrasonography Journal 1/2023Document132 pagesMedical Ultrasonography Journal 1/2023nihilx27374No ratings yet
- 93306Document64 pages93306jamesgailNo ratings yet
- LiverultrasoundDocument62 pagesLiverultrasoundiuliia94No ratings yet
- Color and Power DopplerDocument114 pagesColor and Power DopplerThuraiya Al MasoudiNo ratings yet
- Ob Biophysical Profile Protocol r14 PDFDocument3 pagesOb Biophysical Profile Protocol r14 PDFapi-390240132No ratings yet
- Quantification of Severity of Mitral Regurgitation With The New ASE GuidelinesDocument20 pagesQuantification of Severity of Mitral Regurgitation With The New ASE GuidelinesPanfilAlinaNo ratings yet
- Abdominal US in Hepatobiliary DiseasesDocument76 pagesAbdominal US in Hepatobiliary DiseasesSyafari D. MangopoNo ratings yet
- Principlesofdopplerultrasound 130514165605 Phpapp02Document92 pagesPrinciplesofdopplerultrasound 130514165605 Phpapp02csngiu100% (2)
- Policies and Statements: Peripheral Arterial UltrasoundDocument5 pagesPolicies and Statements: Peripheral Arterial UltrasoundJing CruzNo ratings yet
- 14 Clauss Pediatric Echocardiography PDFDocument159 pages14 Clauss Pediatric Echocardiography PDFSergiu NiculitaNo ratings yet
- Echo KibuddeDocument54 pagesEcho KibuddeTrevor Ishmael SiakambaNo ratings yet
- ASE HCM Poster FINALDocument2 pagesASE HCM Poster FINALBandar Alamri100% (1)
- Ultrasound EchocardiographyDocument3 pagesUltrasound EchocardiographyDr. MLKNo ratings yet
- Introduction, Physics and KnobologyDocument47 pagesIntroduction, Physics and KnobologyMihaela LoghinNo ratings yet
- Ultrasound: Made By: Conny LeoDocument15 pagesUltrasound: Made By: Conny LeoChristabelle ConnyNo ratings yet
- Real-Time 3D EchocardiographyDocument159 pagesReal-Time 3D Echocardiographymalvina902009No ratings yet
- Kuliah Blok GI Tract - USG Abd - September 2010Document65 pagesKuliah Blok GI Tract - USG Abd - September 2010Natallia BatuwaelNo ratings yet
- Abdomen Protocol 14 PDFDocument6 pagesAbdomen Protocol 14 PDFapi-390240132No ratings yet
- Lvot o IiDocument179 pagesLvot o Iimona300No ratings yet
- Diastolic DysfunctionDocument6 pagesDiastolic DysfunctionMarina SecureanuNo ratings yet
- Vascular Disorders StudentsDocument70 pagesVascular Disorders StudentsedwinNo ratings yet
- Guidelines of Arterial Duplex ScanDocument23 pagesGuidelines of Arterial Duplex ScanMohamed Omar Elfarok100% (1)
- Penile US and Doppler USDocument2 pagesPenile US and Doppler UShardrocker_2007No ratings yet
- EACVI Multimodality Imaging of Native Valvular RegDocument62 pagesEACVI Multimodality Imaging of Native Valvular RegВенцислав МирчевNo ratings yet
- Gynecoloical Ultrasound Doppler AssessmentDocument17 pagesGynecoloical Ultrasound Doppler AssessmentKinzaNo ratings yet
- Arterial DopplerDocument29 pagesArterial DopplerAudrey100% (20)
- Adult Echocardiography Protocol 14 2Document10 pagesAdult Echocardiography Protocol 14 2api-349402240No ratings yet
- Unit 1 Basics of Echocardiography and Cardiac DopplerDocument29 pagesUnit 1 Basics of Echocardiography and Cardiac DopplerJack TomarNo ratings yet
- Pediatric Spine 14Document2 pagesPediatric Spine 14api-349402240No ratings yet
- Biophysical Profile& Color Doppler Ultrasound in The High Risk PregnancyDocument56 pagesBiophysical Profile& Color Doppler Ultrasound in The High Risk Pregnancykhadzx100% (4)
- D5 PolicyDocument5 pagesD5 PolicyDenis PogoreviciNo ratings yet
- Prosth ValvesDocument74 pagesProsth ValvesRavi ZoreNo ratings yet
- Usg Blok 17Document104 pagesUsg Blok 17iqiqiqiqiqNo ratings yet
- Us Vasos RetroperitonealesDocument101 pagesUs Vasos RetroperitonealesLourdes MarcosNo ratings yet
- Ultrasonography Assessment of Lower Limb VeinsDocument49 pagesUltrasonography Assessment of Lower Limb VeinsPutra AchmadNo ratings yet
- Lower Extremity Venous Protocol 14Document3 pagesLower Extremity Venous Protocol 14api-349474075No ratings yet
- Carotid Protocol 14 1Document4 pagesCarotid Protocol 14 1api-349402240No ratings yet
- Fetal Echocardiogram ProtocolDocument4 pagesFetal Echocardiogram Protocolapi-349402240No ratings yet
- Allen Test Protocol 14 1Document2 pagesAllen Test Protocol 14 1api-349402240No ratings yet
- Pediatric Spine 14Document2 pagesPediatric Spine 14api-349402240No ratings yet
- Adult Echocardiography Protocol 14 2Document10 pagesAdult Echocardiography Protocol 14 2api-349402240No ratings yet
- Scrotum Protocol 14Document2 pagesScrotum Protocol 14api-349402240No ratings yet
- Abdomen ProtocolDocument8 pagesAbdomen Protocolapi-349474075No ratings yet
- Liver Protocol 14 1Document5 pagesLiver Protocol 14 1api-349402240No ratings yet
- Appendix Protocol 14 1Document2 pagesAppendix Protocol 14 1api-349402240No ratings yet
- ECG Interpretation in Small AnimalsDocument10 pagesECG Interpretation in Small Animalsgacf1974No ratings yet
- Administering Metoprolol IV Push 1Document22 pagesAdministering Metoprolol IV Push 1api-357388170No ratings yet
- Echocardiography Juni 2018Document1 pageEchocardiography Juni 2018Prima Agung LNo ratings yet
- Circulatory SystemDocument2 pagesCirculatory SystemGlen MillarNo ratings yet
- VF-VT AlgorithmDocument10 pagesVF-VT AlgorithmPuskesmas Pinang JayaNo ratings yet
- HypertensionDocument8 pagesHypertensionMario MorinNo ratings yet
- Amaurosis FugaxDocument12 pagesAmaurosis FugaxSubashini G DeviNo ratings yet
- Early Complications of MIDocument11 pagesEarly Complications of MIjen262004No ratings yet
- Farm TocliDocument3 pagesFarm TocliPankaj MaithaniNo ratings yet
- Program Book of INAechoDocument15 pagesProgram Book of INAechoAnthomina MayaNo ratings yet
- Accreditation in Adult Transthoracic Echocardiography (TTE) Information PackDocument57 pagesAccreditation in Adult Transthoracic Echocardiography (TTE) Information PackJoseph BarkerNo ratings yet
- Circulatory System REVIEWERDocument6 pagesCirculatory System REVIEWERClyde BaltazarNo ratings yet
- Vein ChartDocument5 pagesVein ChartThomasNo ratings yet
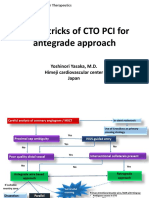
- Tips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanDocument21 pagesTips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanEll KlazureNo ratings yet
- Arterial Cannulation A Critical ReviewDocument5 pagesArterial Cannulation A Critical ReviewYoel PurnamaNo ratings yet
- Jessica Newton Imaging Technologies February 2, 2011Document3 pagesJessica Newton Imaging Technologies February 2, 2011jnewton4No ratings yet
- MCQ Cardio 2Document54 pagesMCQ Cardio 2Dian Paramita100% (1)
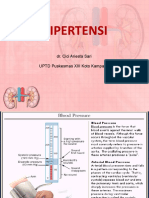
- Hipertensi: Dr. Cici Ariesta Sari UPTD Puskesmas XIII Koto Kampar IDocument25 pagesHipertensi: Dr. Cici Ariesta Sari UPTD Puskesmas XIII Koto Kampar ICici AriestaNo ratings yet
- Kelompok 3Document30 pagesKelompok 3adityaNo ratings yet
- Cases in Cardio PediatricDocument298 pagesCases in Cardio Pediatricmarie saul100% (3)
- SSS, BCS, Avf, MalDocument42 pagesSSS, BCS, Avf, MalchintamaniNo ratings yet
- Circulatory System NotesDocument8 pagesCirculatory System Notesthe lillyNo ratings yet
- Burger Allen Exercises PDFDocument122 pagesBurger Allen Exercises PDFlucky 116No ratings yet
- CCN 1Document9 pagesCCN 1Shafiq Ur RahmanNo ratings yet
- EmbolismDocument2 pagesEmbolismShannen Joyce FloresNo ratings yet
- Guyton at The BedsideDocument7 pagesGuyton at The BedsideGustavo ParedesNo ratings yet
- Electrofisiologia Cardiaca Guia Viasual 2 PDFDocument82 pagesElectrofisiologia Cardiaca Guia Viasual 2 PDFMiguel LizarragaNo ratings yet
- Circulatory System HandoutsDocument4 pagesCirculatory System HandoutsCzarae VillanuevaNo ratings yet
- CCrISP 7 Shock and HaemorrhageDocument27 pagesCCrISP 7 Shock and HaemorrhageDrSayk YousufNo ratings yet
- Indikasi TrombektomiDocument6 pagesIndikasi TrombektomiNatasha BastiaanNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (30)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (5)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainFrom EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainRating: 4 out of 5 stars4/5 (95)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (61)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (60)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (45)