You might also like
- CHG To Ssi PDFDocument7 pagesCHG To Ssi PDFDian RahmawatiNo ratings yet
- Final Research PaperDocument9 pagesFinal Research Paperapi-444947174No ratings yet
- Vondessauer 2016Document7 pagesVondessauer 2016زينب محمد عبدNo ratings yet
- Antiseptic Synthesis of Evidence-2Document8 pagesAntiseptic Synthesis of Evidence-2api-673177967No ratings yet
- The Effectiveness of Chlorhexidine Bathing in The Prevention of ClabsisDocument9 pagesThe Effectiveness of Chlorhexidine Bathing in The Prevention of Clabsisapi-576596429No ratings yet
- Surgical Site InfectionDocument7 pagesSurgical Site InfectionCaxton ThumbiNo ratings yet
- CholeraDocument7 pagesCholeraDewa Ayu Pradnya DewiNo ratings yet
- Medi 100 E25304Document5 pagesMedi 100 E25304Nurul AidaNo ratings yet
- Mukherjee 2017Document8 pagesMukherjee 2017mark perezNo ratings yet
- Solis Antisépticos ArtDocument1 pageSolis Antisépticos ArtYENNY DEL CARMEN SOLÍS BAEZANo ratings yet
- Resistencia ClorhexidinaDocument30 pagesResistencia ClorhexidinaVlady78No ratings yet
- UntitledDocument7 pagesUntitledherdian ariebowoNo ratings yet
- ProkalsitoninDocument11 pagesProkalsitoninFarmasi RSUD Kramat JatiNo ratings yet
- Rcse9505 345Document4 pagesRcse9505 345Swekshya PandeyNo ratings yet
- Colistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM EvidenceDocument27 pagesColistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM Evidencerac.oncologyNo ratings yet
- Does An Antimicrobial Incision Drape Prevent.15Document9 pagesDoes An Antimicrobial Incision Drape Prevent.15Jimenez-Espinosa JeffersonNo ratings yet
- Farmakokinetik EnroDocument12 pagesFarmakokinetik EnrokarjonoNo ratings yet
- Ebp Formative Synthesis PaperDocument9 pagesEbp Formative Synthesis Paperapi-404415990No ratings yet
- American Journal of Infection ControlDocument6 pagesAmerican Journal of Infection ControlAuliasari SiskaNo ratings yet
- Efficacy and Safety of Broad Spectrum Penicillin With or Without Beta Lactamase Inhibitors Vs First and Second Generation Cephalosporins AsDocument10 pagesEfficacy and Safety of Broad Spectrum Penicillin With or Without Beta Lactamase Inhibitors Vs First and Second Generation Cephalosporins AsKhairun nisaNo ratings yet
- Deshpande2018 PDFDocument5 pagesDeshpande2018 PDFSixth Batch PharmacyNo ratings yet
- 1 s2.0 S0195670118305425 MainDocument4 pages1 s2.0 S0195670118305425 MainMuhammad Cholid AlfahroziNo ratings yet
- Journal Club: Presented by Ali Al-Zahir GS ResidentDocument27 pagesJournal Club: Presented by Ali Al-Zahir GS ResidentAli AlzahirNo ratings yet
- Journal of Clinical Microbiology-2011-Wolk-S62.fullDocument6 pagesJournal of Clinical Microbiology-2011-Wolk-S62.fullAli AhmedNo ratings yet
- Antibiotics 11 00022Document16 pagesAntibiotics 11 00022Putri RamadhaniNo ratings yet
- Effect of Daily Chlorhexidine Bathing On Hospital-Acquired InfectionDocument10 pagesEffect of Daily Chlorhexidine Bathing On Hospital-Acquired InfectionKanameMizumiNo ratings yet
- 1 s2.0 S0039606018302721 MainDocument7 pages1 s2.0 S0039606018302721 MainMelo Pérez Pamela J.No ratings yet
- Feasibility of Eliminating Ocular Chlamydia Trachomatis With Repeat Mass Antibiotic TreatmentsDocument5 pagesFeasibility of Eliminating Ocular Chlamydia Trachomatis With Repeat Mass Antibiotic TreatmentsAmelia RoziantyNo ratings yet
- Facemasks and Hand Hygiene To Prevent Influenza TR PDFDocument21 pagesFacemasks and Hand Hygiene To Prevent Influenza TR PDFTiudusNo ratings yet
- Chlorhexidine-Alcohol Compared With Povidone-Iodine Preoperative Skin Antisepsis For Cesarean Delivery A Systematic Review and Meta-AnalysisDocument6 pagesChlorhexidine-Alcohol Compared With Povidone-Iodine Preoperative Skin Antisepsis For Cesarean Delivery A Systematic Review and Meta-AnalysisjohnturpoNo ratings yet
- Jurnal Vaksin BCG 2Document9 pagesJurnal Vaksin BCG 2niken ambarNo ratings yet
- Topical Antibiotics To Prevent Surgical Site Infection After Minor Surgery in Primary CareDocument5 pagesTopical Antibiotics To Prevent Surgical Site Infection After Minor Surgery in Primary CarePitchya WangmeesriNo ratings yet
- Pi Is 0196064409002704Document7 pagesPi Is 0196064409002704adesamboraNo ratings yet
- Right To Refuse Flu ShotsDocument4 pagesRight To Refuse Flu ShotsBZ Riger100% (2)
- Elevating The Standard of Endoscope Processing Terminal Sterilization of Duodenoscopes Using A Hydrogenperoxide Ozone SterilizerDocument8 pagesElevating The Standard of Endoscope Processing Terminal Sterilization of Duodenoscopes Using A Hydrogenperoxide Ozone SterilizerMicro SoftNo ratings yet
- The Combined Impact of Surgical Team Education and Chlorhexidine 2% Alcohol On The Reduction of Surgical Site Infection Following Cardiac SurgeryDocument7 pagesThe Combined Impact of Surgical Team Education and Chlorhexidine 2% Alcohol On The Reduction of Surgical Site Infection Following Cardiac SurgeryShandaPrimaDewiNo ratings yet
- Povidone-Iodine Vs Chlorhexidine Alcohol For Skin Preparation in Malignant and Premalignant Gynaecologic Diseases A RanDocument8 pagesPovidone-Iodine Vs Chlorhexidine Alcohol For Skin Preparation in Malignant and Premalignant Gynaecologic Diseases A RanTri Dhani AnandaNo ratings yet
- ATB Gyne PDFDocument10 pagesATB Gyne PDFNATTAPAT SANGKAKULNo ratings yet
- Chlorhexidine Vs Tincture of Iodine For ReductionDocument4 pagesChlorhexidine Vs Tincture of Iodine For Reductionmohamad mansurNo ratings yet
- A Study On Resistance Pattern of Bacteria Isolated From Diabetic and Non - Diabetic UlcersDocument7 pagesA Study On Resistance Pattern of Bacteria Isolated From Diabetic and Non - Diabetic UlcersBIOMEDSCIDIRECT PUBLICATIONSNo ratings yet
- Procalcitonin and AB DecisionsDocument10 pagesProcalcitonin and AB DecisionsDennysson CorreiaNo ratings yet
- Pone 0129434Document15 pagesPone 0129434api-325197812No ratings yet
- Articulo 7Document7 pagesArticulo 7Janet CastilloNo ratings yet
- Critical Care InfectionDocument15 pagesCritical Care InfectionTito Ahmad RizkiawanNo ratings yet
- 4147 15918 1 PBDocument7 pages4147 15918 1 PBI Made AryanaNo ratings yet
- A Review On Antibiotic Resistance in BacteriaDocument9 pagesA Review On Antibiotic Resistance in BacteriaIJRASETPublicationsNo ratings yet
- 1471 2334 11 278Document6 pages1471 2334 11 278Dwi WirastomoNo ratings yet
- 04 Iajps04062017Document9 pages04 Iajps04062017Baru Chandrasekhar RaoNo ratings yet
- BJMP 2012 5 1 A512Document5 pagesBJMP 2012 5 1 A512maslikanNo ratings yet
- Chenodeoxycholic Acid-Amikacin Combination Enhances ERradication of StaphyDocument17 pagesChenodeoxycholic Acid-Amikacin Combination Enhances ERradication of StaphyAlex HernandezNo ratings yet
- Aborto Septico 2020Document5 pagesAborto Septico 2020Adrian Pardo VillegasNo ratings yet
- GammaglobulinaDocument7 pagesGammaglobulinaIván Gustavo Magaña CeballosNo ratings yet
- ATB ProfilaxisDocument10 pagesATB Profilaxiscristopher_ahcNo ratings yet
- Chitosan Nanoparticles PHD ThesisDocument6 pagesChitosan Nanoparticles PHD Thesisfjgmmmew100% (2)
- Effectiveness of Surgical Hand Antisepsis Using Chlorhexidine Digluconate and Parachlorometaxylenol Hand ScrubDocument6 pagesEffectiveness of Surgical Hand Antisepsis Using Chlorhexidine Digluconate and Parachlorometaxylenol Hand ScrubJuan Vaca GonzálezNo ratings yet
- American Journal of Infection ControlDocument8 pagesAmerican Journal of Infection ControlRizky AdipratamaNo ratings yet
- The Efficacy of Daily Chlorhexidine Bathing For Preventing Healthcare-Associated Infections in Adult Intensive Care UnitsDocument12 pagesThe Efficacy of Daily Chlorhexidine Bathing For Preventing Healthcare-Associated Infections in Adult Intensive Care UnitsKanameMizumiNo ratings yet
- Cetylpyridinium Chloride CPC Exhibits Potent RapidDocument18 pagesCetylpyridinium Chloride CPC Exhibits Potent RapidchitarraNo ratings yet
- Psychoneuroimmunology - Laugh and Be Well - Medical News TodayDocument6 pagesPsychoneuroimmunology - Laugh and Be Well - Medical News TodayBarbara Sakura RiawanNo ratings yet
- Useful Medications For Oral Conditions: AnalgesicsDocument8 pagesUseful Medications For Oral Conditions: AnalgesicsnewmexicoomfsNo ratings yet
- Original Contributions: Stroke: Highlights of Selected ArticlesDocument7 pagesOriginal Contributions: Stroke: Highlights of Selected ArticlesBarbara Sakura RiawanNo ratings yet
- Dietary Essential Fatty Acids and Brain Function A Developmental Perspective On MechanismsDocument9 pagesDietary Essential Fatty Acids and Brain Function A Developmental Perspective On MechanismsBarbara Sakura RiawanNo ratings yet
- Dietary Essential Fatty Acids and Brain Function A Developmental Perspective On MechanismsDocument9 pagesDietary Essential Fatty Acids and Brain Function A Developmental Perspective On MechanismsBarbara Sakura RiawanNo ratings yet
- Aria Rhinitis Allergic Pocket GuideDocument8 pagesAria Rhinitis Allergic Pocket GuideAlfani FajarNo ratings yet
- Lotus Birth Associated With Idiopathic Neonatal Hepatitis: SciencedirectDocument2 pagesLotus Birth Associated With Idiopathic Neonatal Hepatitis: SciencedirectBarbara Sakura RiawanNo ratings yet
- Complication of Regional AnestesiaDocument10 pagesComplication of Regional AnestesiaBarbara Sakura RiawanNo ratings yet
- HTN4Document9 pagesHTN4Barbara Sakura RiawanNo ratings yet
- Harg A Ubiqui NoneDocument2 pagesHarg A Ubiqui NoneBarbara Sakura RiawanNo ratings yet
- Ace InhibitorsDocument20 pagesAce InhibitorsArif Abdul HaiNo ratings yet
- Article 61 enDocument3 pagesArticle 61 enBarbara Sakura RiawanNo ratings yet
- 1 - 2013guidelines (1) - ATC PDFDocument284 pages1 - 2013guidelines (1) - ATC PDFrini setyawatiNo ratings yet
- Am J Clin Nutr 2016 Taylor 1647 56Document10 pagesAm J Clin Nutr 2016 Taylor 1647 56Barbara Sakura RiawanNo ratings yet
- How to Fold Paper ProperlyDocument1 pageHow to Fold Paper ProperlyBarbara Sakura RiawanNo ratings yet
- AUA Guidelines of BPHDocument54 pagesAUA Guidelines of BPHnntclaytonNo ratings yet
- Ace InhibitorsDocument20 pagesAce InhibitorsArif Abdul HaiNo ratings yet
- Thyroid CancerDocument13 pagesThyroid CancerBarbara Sakura RiawanNo ratings yet
- V 080 P 00634Document8 pagesV 080 P 00634Barbara Sakura RiawanNo ratings yet
- Ni Hms 240769Document17 pagesNi Hms 240769Barbara Sakura RiawanNo ratings yet
- 454 FullDocument8 pages454 FullBarbara Sakura RiawanNo ratings yet
- 1 s2.0 S0168827810005647 Main PDFDocument7 pages1 s2.0 S0168827810005647 Main PDFBarbara Sakura RiawanNo ratings yet
- JHH 201654 ADocument11 pagesJHH 201654 ABarbara Sakura RiawanNo ratings yet
- JHH 200977 ADocument11 pagesJHH 200977 ABarbara Sakura RiawanNo ratings yet
- HOPEDocument21 pagesHOPEBarbara Sakura RiawanNo ratings yet
- Hemodynamic Response To Pharmacological Treatment of Portal Hypertension and Long-Term Prognosis of CirrhosisDocument7 pagesHemodynamic Response To Pharmacological Treatment of Portal Hypertension and Long-Term Prognosis of CirrhosisBarbara Sakura RiawanNo ratings yet
- Complication of Regional AnestesiaDocument10 pagesComplication of Regional AnestesiaBarbara Sakura RiawanNo ratings yet
- Management of Cirrhosis and Portal Hypertension - 2009Document28 pagesManagement of Cirrhosis and Portal Hypertension - 2009BENNo ratings yet
- Feline Herpes VirusDocument10 pagesFeline Herpes Viruskadek ayu ichaNo ratings yet
- Antibacterial Activity Assay Protocol - Minimum Inhibitory ConcentrationDocument7 pagesAntibacterial Activity Assay Protocol - Minimum Inhibitory ConcentrationAngela BanerjeeNo ratings yet
- Guide To Infection Control in The Hospital: Hand HygieneDocument11 pagesGuide To Infection Control in The Hospital: Hand HygieneSlepy chngNo ratings yet
- AGR514 Chapter 1Document23 pagesAGR514 Chapter 1Muhamad Afif Abdul FatahNo ratings yet
- HIV Vaccines Overview: Shaleena TheophilusDocument34 pagesHIV Vaccines Overview: Shaleena TheophilusREETHUNo ratings yet
- Module SC f5 p2 CHAPTER 1Document10 pagesModule SC f5 p2 CHAPTER 1norasiah6500No ratings yet
- Virology The Study of VirusesDocument45 pagesVirology The Study of Virusesdawoodabdullah56100% (2)
- Types of Influenza VirusesDocument105 pagesTypes of Influenza Virusesjohn dadisNo ratings yet
- Oxygen 2222Document75 pagesOxygen 2222Salim AlmetewtyNo ratings yet
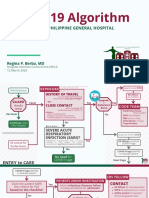
- COVID-19 Algorithm: For The Philippine General HospitalDocument10 pagesCOVID-19 Algorithm: For The Philippine General HospitalJay VeeNo ratings yet
- Immunization Seminar BenefitsDocument42 pagesImmunization Seminar BenefitsRionaMarieMagbutay67% (3)
- ANTIBACTERIAL ACTIVITY of GARLIC (Allium Sativum L.)Document10 pagesANTIBACTERIAL ACTIVITY of GARLIC (Allium Sativum L.)Tiyas YassNo ratings yet
- Government of Telangana Covid Interim Test Report CCMB, HyderabadDocument2 pagesGovernment of Telangana Covid Interim Test Report CCMB, HyderabadNagarjunaNo ratings yet
- Determinant Factors That Influence The Prevalence of Gonorrhea in Female Sex Wokers in YogyakartaDocument12 pagesDeterminant Factors That Influence The Prevalence of Gonorrhea in Female Sex Wokers in YogyakartaSiti MaesarohNo ratings yet
- Pamantasan NG Lungsod NG MaynilaDocument4 pagesPamantasan NG Lungsod NG MaynilatipyangNo ratings yet
- Submerged Culture of The Mycelium of Various Species of MushroomDocument3 pagesSubmerged Culture of The Mycelium of Various Species of Mushroombravohr98No ratings yet
- Classifying of MicroorganismsDocument26 pagesClassifying of MicroorganismsDaman Huri WibowoNo ratings yet
- 157-Article Text-629-1-10-20230331Document7 pages157-Article Text-629-1-10-20230331Dyah tantri WNo ratings yet
- Bacteremia - Blood Cultures and Other Diagnostic Tools - UpToDateDocument15 pagesBacteremia - Blood Cultures and Other Diagnostic Tools - UpToDateJota MartinezNo ratings yet
- Emerging & Re-emerging infectious Diseases: New ThreatsDocument68 pagesEmerging & Re-emerging infectious Diseases: New ThreatsIwan Purnawan100% (1)
- HIV To Draw DiagramDocument1 pageHIV To Draw DiagramShantonil BalNo ratings yet
- USMLE Step 1 First Aid 2020 30th - MICROBIOLOGYDocument82 pagesUSMLE Step 1 First Aid 2020 30th - MICROBIOLOGYArt PuffNo ratings yet
- Ubiquidad y distribución de los microorganismosDocument6 pagesUbiquidad y distribución de los microorganismosLeonardoEscalante100% (1)
- Endometritis BrochureDocument2 pagesEndometritis BrochureNovelyn PuaNo ratings yet
- E-Poster Veena PillaiDocument1 pageE-Poster Veena PillaiVeena PillaiNo ratings yet
- Asepsis 1Document52 pagesAsepsis 1严子明 Renz Ryan SevillenoNo ratings yet
- SGD Case Presentation 10Document26 pagesSGD Case Presentation 10Karen C. Del RosarioNo ratings yet
- Infection Control CommitteeDocument7 pagesInfection Control Committeefarha naazNo ratings yet
- What Is Chikungunya Virus?Document12 pagesWhat Is Chikungunya Virus?Quenzil LumodNo ratings yet
- Fistula in AnoDocument14 pagesFistula in AnoManinithya KalvakotaNo ratings yet