You might also like
- Soal Ujian Bedah SarafDocument7 pagesSoal Ujian Bedah SarafdrghempikNo ratings yet
- MCQ Neuro SampleDocument12 pagesMCQ Neuro SampleMutiara AdystiNo ratings yet
- Fracp Past Papers - NeurologyDocument21 pagesFracp Past Papers - NeurologyLakshya J BasumataryNo ratings yet
- Neurosurgery Past PapersDocument74 pagesNeurosurgery Past PapersRand AhmadNo ratings yet
- 2011-2012 Group 6Document5 pages2011-2012 Group 6Law YouNo ratings yet
- Neurosurgery MCQ'sDocument5 pagesNeurosurgery MCQ'sRajanish Kumar50% (2)
- Formative Assessment FinalDocument5 pagesFormative Assessment FinalJonathan YeohNo ratings yet
- Neuro TestDocument9 pagesNeuro TestHanung MerahbaraNo ratings yet
- Rle Rot 2Document4 pagesRle Rot 2Da BondadNo ratings yet
- Kumpulan Soal 1Document25 pagesKumpulan Soal 1Muhammad Azhary LazuardyNo ratings yet
- Seleksi Imo SoalDocument11 pagesSeleksi Imo SoalOlga FannyNo ratings yet
- Trauma Kapitis RevisiDocument54 pagesTrauma Kapitis RevisiRatika Ayu PiliangNo ratings yet
- Trauma KepalaDocument43 pagesTrauma KepalaAray Al-AfiqahNo ratings yet
- Neurology SAUDI EXAM 1Document19 pagesNeurology SAUDI EXAM 1Asif Newaz100% (2)
- NerosurgeryDocument34 pagesNerosurgeryapi-19502000100% (1)
- Head Injury ManagementDocument11 pagesHead Injury Managementrajan kumar100% (1)
- Soal AAO PO Chapter 18Document3 pagesSoal AAO PO Chapter 18Defayudina Dafilianty RosatariaNo ratings yet
- Brain Resuscitation and Protection MutiaraDocument30 pagesBrain Resuscitation and Protection MutiaraMutiaraNo ratings yet
- HSC 3.5Document206 pagesHSC 3.5friscaNo ratings yet
- Neuro FinalDocument70 pagesNeuro FinalOmar HatemNo ratings yet
- Diagnosis - AksisDocument4 pagesDiagnosis - AksisAbdi Wahyu NurdiansyahNo ratings yet
- Bedah Anak Lanjut Pilihan GandaDocument1 pageBedah Anak Lanjut Pilihan GandaGilberto ChafrinaNo ratings yet
- Neurology Unanswered (1700q Unity Order) PDFDocument32 pagesNeurology Unanswered (1700q Unity Order) PDFNeha GoelNo ratings yet
- Final-Exam Neurosurgery - 2-VersionDocument6 pagesFinal-Exam Neurosurgery - 2-VersionMAMA LALANo ratings yet
- 11 Neurology PDFDocument17 pages11 Neurology PDFalialison7666100% (1)
- Contoh Soal RMDocument5 pagesContoh Soal RMAlbert PriadiNo ratings yet
- Arab Board Final 2018 - 2Document12 pagesArab Board Final 2018 - 2lonsilord17No ratings yet
- General AnaesthesiaDocument53 pagesGeneral Anaesthesiapeter singal100% (2)
- Jurnal MRCPDocument18 pagesJurnal MRCPMaharani Eka SaputriNo ratings yet
- Soal OrthopediDocument3 pagesSoal OrthopediPoppy GhufraniNo ratings yet
- Blueprints QA Pediatrics For Step 3 1Document59 pagesBlueprints QA Pediatrics For Step 3 1Moataz Trabeh100% (1)
- Trauma and Burns MCQDocument74 pagesTrauma and Burns MCQAhmed Kassem100% (2)
- NeurosurgeryDocument1 pageNeurosurgeryNiko MelialaNo ratings yet
- Soal RetinaDocument2 pagesSoal RetinadrheriNo ratings yet
- Neuroscience FK UPH 2014: Multiple Choice QuestionsDocument33 pagesNeuroscience FK UPH 2014: Multiple Choice QuestionsSanzuiNo ratings yet
- 18 - Trauma in ElderlyDocument18 pages18 - Trauma in ElderlyIman KadeNo ratings yet
- Neurosurgery Final Exam (M.@) - M@Jed Al@MiDocument5 pagesNeurosurgery Final Exam (M.@) - M@Jed Al@MiIbrahem Y. Najjar100% (1)
- Neurology MCQDocument5 pagesNeurology MCQRaghu Nadh0% (1)
- ExamDocument8 pagesExamkrull243No ratings yet
- Anatomical Basis of Cranial Neurosurgery (PDFDrive)Document463 pagesAnatomical Basis of Cranial Neurosurgery (PDFDrive)Alkawthar M. AbdulsadaNo ratings yet
- Principals of Cranial Surgery For Tumors MCQ-1Document9 pagesPrincipals of Cranial Surgery For Tumors MCQ-1lonsilord17100% (1)
- Saudi Board Question Bank PDFDocument414 pagesSaudi Board Question Bank PDFbwaey100% (2)
- Benedict SyndromeDocument5 pagesBenedict SyndromeMarthin Fernandes PasaribuNo ratings yet
- Soal Pretes Calon PPDS Ilmu Bedah SarafDocument6 pagesSoal Pretes Calon PPDS Ilmu Bedah SarafdewiNo ratings yet
- A. Atresia Surgery On at Least One Ear by Age 3 Years: B. Bone-Anchored Hearing Aid (BAHA) Soft BandDocument37 pagesA. Atresia Surgery On at Least One Ear by Age 3 Years: B. Bone-Anchored Hearing Aid (BAHA) Soft Bandevamirandafitri19No ratings yet
- ASIA ScoreDocument2 pagesASIA ScoreIqbal BaryarNo ratings yet
- Neurosurgery Question BankDocument2 pagesNeurosurgery Question BankYoussry Jaranilla40% (5)
- Teaching MCQ-Neurology BasicsDocument17 pagesTeaching MCQ-Neurology Basicslonsilord17No ratings yet
- Rehabilitation Interventions For Postintensive Care Syndrome A Systematic A Review - Mehlhorn2014Document10 pagesRehabilitation Interventions For Postintensive Care Syndrome A Systematic A Review - Mehlhorn2014RodrigoSachiFreitasNo ratings yet
- 2015 NOV. Final Arabic BoardDocument21 pages2015 NOV. Final Arabic Boardlonsilord17No ratings yet
- 39 MCQ's in NeurosurgeryDocument26 pages39 MCQ's in NeurosurgeryAhmed Hamid Ibrahim100% (4)
- Neuropsychiatry Final MCQDocument6 pagesNeuropsychiatry Final MCQRifqi MuhammadNo ratings yet
- Soal Tes PpdsDocument14 pagesSoal Tes PpdsDuas Jourgie100% (1)
- 5-Neuro MCQs Final UnsolvedDocument29 pages5-Neuro MCQs Final UnsolvedOsman Somi0% (2)
- Cat 8Document6 pagesCat 8rukshnNo ratings yet
- Trauma MCQ DiDocument13 pagesTrauma MCQ DiJohn M. HemsworthNo ratings yet
- C 16Document12 pagesC 16Dharati PatelNo ratings yet
- Y Tube Ipost Test OnlineDocument11 pagesY Tube Ipost Test OnlineMohammed Manassra100% (1)
- Y Tube Ipost Test OnlineDocument13 pagesY Tube Ipost Test OnlineAnnisa Lenggogeni0% (1)
- ATLSDocument4 pagesATLSTerri Sandi Susyanto73% (11)
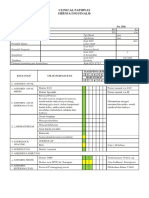
- Clinical Pathway Limphadenopaty ColiDocument6 pagesClinical Pathway Limphadenopaty ColiTina HerreraNo ratings yet
- CP HerniaDocument6 pagesCP HerniaTina HerreraNo ratings yet
- Clinical Pathway Apendisitis AcutaDocument7 pagesClinical Pathway Apendisitis AcutaTina HerreraNo ratings yet
- Jurnal PoneDocument21 pagesJurnal PoneTina HerreraNo ratings yet
- Pie 2018Document5 pagesPie 2018Tina HerreraNo ratings yet
- Tumor Immune Escape Mechanisms: Yi Ting Koh,, M. Luz García-Hernández,, and W. Martin KastDocument26 pagesTumor Immune Escape Mechanisms: Yi Ting Koh,, M. Luz García-Hernández,, and W. Martin KastTina HerreraNo ratings yet
- Wjps 7 016 PDFDocument9 pagesWjps 7 016 PDFTina HerreraNo ratings yet
- Brain Protection, M.Ramli PDFDocument50 pagesBrain Protection, M.Ramli PDFTina HerreraNo ratings yet
- Teks Lagu NatalDocument4 pagesTeks Lagu NatalTina HerreraNo ratings yet
- Intracranial Pathophysiology, Zainal MDocument25 pagesIntracranial Pathophysiology, Zainal MTina HerreraNo ratings yet
- Brain Protection, M.Ramli PDFDocument50 pagesBrain Protection, M.Ramli PDFTina HerreraNo ratings yet
- Thoracic Lumbar, Eko AgusDocument32 pagesThoracic Lumbar, Eko AgusTina HerreraNo ratings yet
- Biomelecular Aspect, Irawan YusufDocument23 pagesBiomelecular Aspect, Irawan YusufTina HerreraNo ratings yet
- Template EnglishDocument15 pagesTemplate EnglishTina HerreraNo ratings yet
- 09.daftar Pustaka FixDocument4 pages09.daftar Pustaka FixTina HerreraNo ratings yet
- Kurnia Ari / 23 THN / MR: 16020635 Admission: 01-02-2016 Consultant: Dr. Almahitta, Spbp-ReDocument7 pagesKurnia Ari / 23 THN / MR: 16020635 Admission: 01-02-2016 Consultant: Dr. Almahitta, Spbp-ReTina HerreraNo ratings yet
- A Guide To Maintenance Metrics-ProgramDocument5 pagesA Guide To Maintenance Metrics-ProgramLy QuanNo ratings yet
- Video Wall, Digital Signage & C'Type Serial NumberDocument8 pagesVideo Wall, Digital Signage & C'Type Serial NumberAbhijit BarmanNo ratings yet
- The Foods of Italy BookDocument92 pagesThe Foods of Italy BookmanupopNo ratings yet
- Corrosion Resistant Steels: Stainless Steel AlloysDocument11 pagesCorrosion Resistant Steels: Stainless Steel AlloysPraveen SamarthiNo ratings yet
- S934 - Instruction ManualDocument36 pagesS934 - Instruction ManualTony MarascaNo ratings yet
- Grade 6 2nd Periodical Test With TOS Answer Keys MATH 1 PDFDocument6 pagesGrade 6 2nd Periodical Test With TOS Answer Keys MATH 1 PDFmafeh caranogNo ratings yet
- YES-O Action-Plan - 2022-2023Document2 pagesYES-O Action-Plan - 2022-2023carmina duldulao100% (6)
- C.E. 324 - Ethics - 1.0Document103 pagesC.E. 324 - Ethics - 1.0dela rosaNo ratings yet
- Igcse ReadingDocument4 pagesIgcse ReadingIvonne PuspakencanaNo ratings yet
- Methodology of Static Pile Load TestDocument33 pagesMethodology of Static Pile Load Testraju_420034520100% (1)
- Smart City Scheme GuidelinesDocument48 pagesSmart City Scheme GuidelinesKarishma Juttun100% (1)
- Method Statement of T-Beams PDFDocument14 pagesMethod Statement of T-Beams PDFKAmi KaMranNo ratings yet
- Dynamic Test Report of DECR-S Excitation Devices: ExperimenterDocument14 pagesDynamic Test Report of DECR-S Excitation Devices: ExperimenterSalmanEjazNo ratings yet
- Factory Program Library List v1.0Document9 pagesFactory Program Library List v1.0Ronaldo DamattaNo ratings yet
- Accesorios Del Lamborghini VenenoDocument31 pagesAccesorios Del Lamborghini VenenoVicente Gil PalopNo ratings yet
- Kids and Their Favourite Food Key Reading Comprehension Exercises - 34436Document2 pagesKids and Their Favourite Food Key Reading Comprehension Exercises - 34436MonicaMartirosyanNo ratings yet
- B11 - Overload Relays (Ref) ENDocument20 pagesB11 - Overload Relays (Ref) ENAhmed AbazaNo ratings yet
- Basic Pancakes Recipe - Martha StewartDocument37 pagesBasic Pancakes Recipe - Martha Stewartkrishna kumarNo ratings yet
- BTS "Whalien 52" Lyrics Romanization, English and Indonesian TranslationDocument11 pagesBTS "Whalien 52" Lyrics Romanization, English and Indonesian TranslationEmaFediFeniNo ratings yet
- kAmAxI Muka Panchashati EngDocument25 pageskAmAxI Muka Panchashati EngSrinathvr100% (1)
- Ap Art and Design Drawing Sustained Investigation Samples 2019 2020 PDFDocument102 pagesAp Art and Design Drawing Sustained Investigation Samples 2019 2020 PDFDominic SandersNo ratings yet
- Gem WK6/WK8 Service ManualDocument18 pagesGem WK6/WK8 Service Manualalex_seidiu100% (5)
- AdsfatreewerwertgdsfDocument1 pageAdsfatreewerwertgdsfJhonel AguilarNo ratings yet
- SuctioningDocument58 pagesSuctioningAyusa PradhanNo ratings yet
- Topic 2 P2: MarkschemeDocument58 pagesTopic 2 P2: MarkschemeZihil ShahNo ratings yet
- Vein Type DepositDocument7 pagesVein Type DepositHarisArmadiNo ratings yet
- Part 7 Mean Field TheoryDocument40 pagesPart 7 Mean Field TheoryOmegaUserNo ratings yet
- COR5500U Series: Digital and CRT Readout OscilloscopeDocument7 pagesCOR5500U Series: Digital and CRT Readout OscilloscopeFlavio FalcãoNo ratings yet
- Lit 1 ReportDocument21 pagesLit 1 ReportTrexie De Vera JaymeNo ratings yet
- Chemistry Lab ReportDocument9 pagesChemistry Lab Reportapi-327824087No ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (29)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (2)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (59)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (45)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)