You might also like
- University of Rizal System: UpperDocument2 pagesUniversity of Rizal System: UpperCes ReyesNo ratings yet
- Emirates FormDocument10 pagesEmirates FormAnonymous B8H5Qq3r100% (1)
- Biology of Orthodontic Tooth MovementsDocument17 pagesBiology of Orthodontic Tooth MovementsDler RaufNo ratings yet
- Cementoenamel Junction An InsightDocument6 pagesCementoenamel Junction An InsightJessica ChenNo ratings yet
- Dental Assisting and Charting Course OutlineDocument4 pagesDental Assisting and Charting Course OutlineShimika TennantNo ratings yet
- Concepts of Enamel and Dentin AdhesionDocument12 pagesConcepts of Enamel and Dentin Adhesionizeldien5870No ratings yet
- Treatment Planning in Operative Dentistry: Dr. Ignatius LeeDocument42 pagesTreatment Planning in Operative Dentistry: Dr. Ignatius LeeDaniel Wang100% (1)
- Caries VaccineDocument19 pagesCaries Vaccinerisana100% (1)
- CARIOLOGY-10.clinical Characteristics of Carious LesionsDocument61 pagesCARIOLOGY-10.clinical Characteristics of Carious LesionsVincent De AsisNo ratings yet
- Lecture 1-Introduction To Dental CariesDocument4 pagesLecture 1-Introduction To Dental CariesAli Al-Qudsi100% (2)
- Dental Enamel: Dr. Prabhat Saxena Dept of Endodontics S.G.T. Dental College, GurgaonDocument114 pagesDental Enamel: Dr. Prabhat Saxena Dept of Endodontics S.G.T. Dental College, GurgaonPrabhat Saxena100% (1)
- Age Changes in Enamel, Dentin and PulpDocument45 pagesAge Changes in Enamel, Dentin and Pulpanmol43% (7)
- Enamel Clinical ConsiderationDocument51 pagesEnamel Clinical ConsiderationBarnali Misra50% (6)
- FCMFOS (SA) Final Past Papers - 2016 2nd Semester 19-4-2018Document1 pageFCMFOS (SA) Final Past Papers - 2016 2nd Semester 19-4-2018Isak Isak IsakNo ratings yet
- EnamelDocument56 pagesEnamelRajesh Jain100% (1)
- Tooth Preparation For AmalgamDocument84 pagesTooth Preparation For AmalgamParidhi GargNo ratings yet
- Library DissertationDocument132 pagesLibrary Dissertationrasagna reddy100% (3)
- 2 - Biologic Consideration of Enamel and Its Clinical Significance in Operative DentistryDocument7 pages2 - Biologic Consideration of Enamel and Its Clinical Significance in Operative DentistryMohammedNo ratings yet
- Caries EtiologyDocument88 pagesCaries EtiologySonalee ShahNo ratings yet
- Abnormalities of Teeth1.2020Document5 pagesAbnormalities of Teeth1.2020Farhaana ShaboodienNo ratings yet
- Last Exams Questions Papers 2018 Dr. Gopika PDFDocument111 pagesLast Exams Questions Papers 2018 Dr. Gopika PDFrhea100% (1)
- Structure of Tooth 2014 ID TopicsDocument24 pagesStructure of Tooth 2014 ID TopicsIsdianaNo ratings yet
- Dental CariesDocument81 pagesDental CariesHusna Hussain100% (1)
- Topic 4Document6 pagesTopic 4Isak Isak IsakNo ratings yet
- Dental Caries Lect 4Document38 pagesDental Caries Lect 4samar yousif mohamedNo ratings yet
- Lecture 2 Caries of EnamelDocument7 pagesLecture 2 Caries of EnamelDt omarNo ratings yet
- 2histopathology of Dental Caries 2Document36 pages2histopathology of Dental Caries 2na huNo ratings yet
- Catatan 20 OktDocument18 pagesCatatan 20 OktAan Mi'dadNo ratings yet
- (RestoDent) Pathophysiology of CariesDocument30 pages(RestoDent) Pathophysiology of CariesZara Sebastianne Garcia100% (1)
- WSLDocument67 pagesWSLSwathyNo ratings yet
- Biologi Struktur Jaringan Keras GigiDocument66 pagesBiologi Struktur Jaringan Keras GigiRhena FitriaNo ratings yet
- Types of Lesion Involved in Tooth DestructionDocument31 pagesTypes of Lesion Involved in Tooth DestructionMustafa SaßerNo ratings yet
- Contemporary Oral and Maxillofacial Surgery - Sapp (Ch. 3)Document24 pagesContemporary Oral and Maxillofacial Surgery - Sapp (Ch. 3)Sebastian GarciaNo ratings yet
- Amelogenesis Imperfecta: Ayesha AwanDocument21 pagesAmelogenesis Imperfecta: Ayesha AwanAyesha AwanNo ratings yet
- Patho Lec 4THDocument3 pagesPatho Lec 4THJane Krystia TeodoroNo ratings yet
- Caries HistopathologyDocument49 pagesCaries Histopathologyimi4No ratings yet
- Presentation of Histopathology of Dental CariesDocument31 pagesPresentation of Histopathology of Dental CariesShumua ShamiNo ratings yet
- 10 Clinical Featuresof Dental CariesDocument47 pages10 Clinical Featuresof Dental Cariesesguerra1901551No ratings yet
- Carious and Non - Carious Lesions Part 1Document23 pagesCarious and Non - Carious Lesions Part 1يوسف حمدNo ratings yet
- Dental Caries Part 2 20207271935560Document25 pagesDental Caries Part 2 20207271935560Ayushi GoelNo ratings yet
- Enamel, Dentin, Pulp Biological ConsiderationDocument41 pagesEnamel, Dentin, Pulp Biological ConsiderationMohammad ANo ratings yet
- All Resto NotesDocument27 pagesAll Resto NotesWinston ZarateNo ratings yet
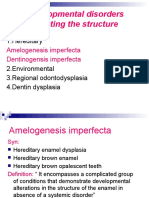
- Developmental Disorders Affecting The StructureDocument59 pagesDevelopmental Disorders Affecting The StructureJerry TurtleNo ratings yet
- OralDocument61 pagesOralPragatiNo ratings yet
- Cariology: Presented By-Dr. Neha Sultana Post Graduate Student Department of Conservative Dentistry and EndodonticsDocument93 pagesCariology: Presented By-Dr. Neha Sultana Post Graduate Student Department of Conservative Dentistry and EndodonticsShailja KatiyarNo ratings yet
- Histopathology of Dental CariesDocument7 pagesHistopathology of Dental CariesJOHN HAROLD CABRADILLANo ratings yet
- UntitledDocument37 pagesUntitledA.Vikram ReddyNo ratings yet
- EnamelDocument139 pagesEnamelA.Vikram ReddyNo ratings yet
- 1965 Martin BrannstromDocument7 pages1965 Martin Brannstrom謎超人No ratings yet
- Week 8 NotesDocument5 pagesWeek 8 NotesDelaney IslipNo ratings yet
- Thuc Hanh R5Document20 pagesThuc Hanh R5sahraNo ratings yet
- Epidemiology 6Document6 pagesEpidemiology 6Batool HusseinNo ratings yet
- L2 Pediatric Operative Dentistry I For Students 18-11-21Document37 pagesL2 Pediatric Operative Dentistry I For Students 18-11-21Ju JuNo ratings yet
- Structure of Teeth: Khushi Desai III BDS 808Document36 pagesStructure of Teeth: Khushi Desai III BDS 808Khushi DesaiNo ratings yet
- Prof. Marium Iqbal Head of Operative Dentistry, Endodontics and PaedodonticsDocument62 pagesProf. Marium Iqbal Head of Operative Dentistry, Endodontics and PaedodonticsumairNo ratings yet
- Lec3 EnamelDocument4 pagesLec3 EnamelGaelle AtNo ratings yet
- Oral Biology AssignmentDocument5 pagesOral Biology AssignmentShaza Khalid0% (1)
- Os MidtermDocument2 pagesOs MidtermGuen ColisNo ratings yet
- EnamelDocument59 pagesEnamelMohammed rezgallahNo ratings yet
- Histologi GigiDocument96 pagesHistologi GigichickenwingsNo ratings yet
- Dentinogenesis Reviewer UwuDocument10 pagesDentinogenesis Reviewer UwuAngierika CorpuzNo ratings yet
- S Tomato LogyDocument37 pagesS Tomato Logyhosam ahmedNo ratings yet
- Odontogenic Tumors IIDocument24 pagesOdontogenic Tumors IIIbn HabibNo ratings yet
- Esthetic Consideration Fixed Dep Credit Hour PRG Shared Course Course Coordinator OperativeDocument39 pagesEsthetic Consideration Fixed Dep Credit Hour PRG Shared Course Course Coordinator OperativeDjoumana BentoumiNo ratings yet
- Dental Caries Classification PDFDocument5 pagesDental Caries Classification PDFTwinamasiko DanielNo ratings yet
- Oral Histology SlidesDocument60 pagesOral Histology SlidesRan And SanNo ratings yet
- 12-Histopathology of Dental CariesDocument43 pages12-Histopathology of Dental CariesLavanya Kalapala100% (1)
- Oh&e Midterm NotesDocument36 pagesOh&e Midterm NotesSHYRE COLEEN CATAYAONo ratings yet
- ProsdentDocument4 pagesProsdentMax PosseltNo ratings yet
- EnamelDocument11 pagesEnamel3ezzat100% (1)
- Course Task - 3 Course (2017) (1453)Document12 pagesCourse Task - 3 Course (2017) (1453)Isak ShatikaNo ratings yet
- FCMFOS (SA) Primary Past Papers - 2016 1st Semester 19-4-2018Document2 pagesFCMFOS (SA) Primary Past Papers - 2016 1st Semester 19-4-2018Isak Isak IsakNo ratings yet
- Testimonial For Student in Arandis DSA203058Document1 pageTestimonial For Student in Arandis DSA203058Isak Isak IsakNo ratings yet
- Guidelines For Presidents and Secretaries of Constituent Colleges 20-4-2018Document5 pagesGuidelines For Presidents and Secretaries of Constituent Colleges 20-4-2018Isak Isak IsakNo ratings yet
- FCMFOS (SA) Regulations 19-4-2018Document17 pagesFCMFOS (SA) Regulations 19-4-2018Isak Isak IsakNo ratings yet
- FCMFOS (SA) Primary Past Papers - 2017 2nd Semester 12-1-2020Document3 pagesFCMFOS (SA) Primary Past Papers - 2017 2nd Semester 12-1-2020yasingamNo ratings yet
- FCMFOS (SA) Primary Past Papers - 2015 2nd Semester 14-6-2017Document2 pagesFCMFOS (SA) Primary Past Papers - 2015 2nd Semester 14-6-2017DEVON BASIL VAN ECKNo ratings yet
- FCMFOS (SA) Primary Past Papers - 2017 1st Semester 12-1-2020Document2 pagesFCMFOS (SA) Primary Past Papers - 2017 1st Semester 12-1-2020yasingamNo ratings yet
- Prevetative TestDocument4 pagesPrevetative TestIsak Isak IsakNo ratings yet
- Developmental DefectsDocument16 pagesDevelopmental DefectsdeenmNo ratings yet
- Histology of Dental PulpDocument9 pagesHistology of Dental PulpIsak Isak IsakNo ratings yet
- FCMFOS (SA) Regulations 19-4-2018Document17 pagesFCMFOS (SA) Regulations 19-4-2018Isak Isak IsakNo ratings yet
- FCMFOS (SA) Intermediate Past Papers - 2014 2nd Semester 19-4-2018Document2 pagesFCMFOS (SA) Intermediate Past Papers - 2014 2nd Semester 19-4-2018Isak Isak IsakNo ratings yet
- Oshana PostsDocument1 pageOshana PostsIsak Isak IsakNo ratings yet
- FCMFOS (SA) Primary Past Papers - 2016 2nd Semester 19-4-2018Document3 pagesFCMFOS (SA) Primary Past Papers - 2016 2nd Semester 19-4-2018Isak Isak IsakNo ratings yet
- FCMFOS (SA) Regulations 19-4-2018Document17 pagesFCMFOS (SA) Regulations 19-4-2018Isak Isak IsakNo ratings yet
- FCMFOS (SA) Final Past Papers - 2018 1st Semester 19-4-2018Document2 pagesFCMFOS (SA) Final Past Papers - 2018 1st Semester 19-4-2018Isak Isak IsakNo ratings yet
- Chapter 12 Cysts of The Jaws - SlidesDocument56 pagesChapter 12 Cysts of The Jaws - SlidesAbiha AliNo ratings yet
- FCMFOS (SA) Primary Past Papers - 2016 2nd Semester 19-4-2018Document3 pagesFCMFOS (SA) Primary Past Papers - 2016 2nd Semester 19-4-2018Isak Isak IsakNo ratings yet
- Fcmfos (Sa) Portfolio 19-4-2018Document24 pagesFcmfos (Sa) Portfolio 19-4-2018Isak Isak IsakNo ratings yet
- The Colleges of Medicine of South Africa: Please Answer Questions 1-4 in A Separate BookDocument3 pagesThe Colleges of Medicine of South Africa: Please Answer Questions 1-4 in A Separate BookIsak Isak IsakNo ratings yet
- The Colleges of Medicine of South Africa: Please Answer Questions 1-3 in One BookDocument3 pagesThe Colleges of Medicine of South Africa: Please Answer Questions 1-3 in One BookIsak Isak IsakNo ratings yet
- FCMFOS (SA) Final Past Papers - 2016 1st Semester 19-4-2018Document2 pagesFCMFOS (SA) Final Past Papers - 2016 1st Semester 19-4-2018Isak Isak IsakNo ratings yet
- FCMFOS (SA) Intermediate Past Papers - 2014 2nd Semester 19-4-2018Document2 pagesFCMFOS (SA) Intermediate Past Papers - 2014 2nd Semester 19-4-2018Isak Isak IsakNo ratings yet
- FCMFOS (SA) Primary Past Papers - 2018 1st Semester 12-1-2020Document11 pagesFCMFOS (SA) Primary Past Papers - 2018 1st Semester 12-1-2020yasingamNo ratings yet
- FCMFOS (SA) Primary Past Papers - 2017 1st Semester 12-1-2020Document2 pagesFCMFOS (SA) Primary Past Papers - 2017 1st Semester 12-1-2020yasingamNo ratings yet
- FCMFOS (SA) Final Past Papers - 2016 1st Semester 19-4-2018Document2 pagesFCMFOS (SA) Final Past Papers - 2016 1st Semester 19-4-2018Isak Isak IsakNo ratings yet
- FCMFOS (SA) Final Past Papers - 2014 2nd Semester 19-4-2018Document2 pagesFCMFOS (SA) Final Past Papers - 2014 2nd Semester 19-4-2018Isak Isak IsakNo ratings yet
- DMFR 20220335Document22 pagesDMFR 20220335Albert CamusNo ratings yet
- Common Dental ProblemsDocument14 pagesCommon Dental ProblemsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Multiple Pulp Polyps Associated With Deciduous TeethDocument4 pagesMultiple Pulp Polyps Associated With Deciduous TeethJea Ayu YogatamaNo ratings yet
- Prof. Marium Iqbal Head of Operative Dentistry, Endodontics and PaedodonticsDocument62 pagesProf. Marium Iqbal Head of Operative Dentistry, Endodontics and PaedodonticsumairNo ratings yet
- Dental CariesDocument4 pagesDental CariesMehdi MoshaveriNo ratings yet
- Translation and Validation of The Arabic Version of The Geriatric Oral Health Assessment Index (GOHAI)Document7 pagesTranslation and Validation of The Arabic Version of The Geriatric Oral Health Assessment Index (GOHAI)Taufiqurrahman Abdul DjabbarNo ratings yet
- Revised Final Business Plan Wwaos Enterprise111 07212021 3 730PMDocument144 pagesRevised Final Business Plan Wwaos Enterprise111 07212021 3 730PMJohn Andrie EscobidoNo ratings yet
- Lect 1 - Part 1. Introduction To Child Health Nursing-2022Document14 pagesLect 1 - Part 1. Introduction To Child Health Nursing-2022LEON HANSNo ratings yet
- Oral HygieneDocument2 pagesOral HygieneprojecybioNo ratings yet
- XEROSTOMIA and BIOXTRA - 2019 - ENDocument34 pagesXEROSTOMIA and BIOXTRA - 2019 - ENVu HuyenNo ratings yet
- Polymers 13 04227Document12 pagesPolymers 13 04227Dhananjay VasuDevaNo ratings yet
- Preoperative Diagnosis of A Third Root Canal in First and Second Maxillary Premolars A Challenge For The ClinicianDocument7 pagesPreoperative Diagnosis of A Third Root Canal in First and Second Maxillary Premolars A Challenge For The ClinicianS S Saad SaadNo ratings yet
- Pulp CapDocument25 pagesPulp CapCatur Putri KinasihNo ratings yet
- 10 3290@j Jad A41630Document16 pages10 3290@j Jad A41630ptoe100% (1)
- New Microsoft Word DocumentDocument3 pagesNew Microsoft Word DocumentHóòdâ SmäîrýNo ratings yet
- Space Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillDocument8 pagesSpace Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillAnonymous JR1VNCNo ratings yet
- G BehavGuide PDFDocument9 pagesG BehavGuide PDFAzi Pertiwi HussainNo ratings yet
- Bio Mechanics of Tooth PreparationDocument151 pagesBio Mechanics of Tooth PreparationJasbrinder Singh TejaNo ratings yet
- Sturdevant's Art and Science of Operative Dentistry - South Asian EditionDocument45 pagesSturdevant's Art and Science of Operative Dentistry - South Asian Editionsharon rajNo ratings yet
- Advanced Caries Microbiota in Teeth With Irreversible PulpitisDocument6 pagesAdvanced Caries Microbiota in Teeth With Irreversible PulpitisAbel PelaezNo ratings yet
- Infant and Child Nutrition: Key PointsDocument4 pagesInfant and Child Nutrition: Key PointsseptiNo ratings yet