You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Ortho Bullets Volume One Trauma 2017Document2,548 pagesOrtho Bullets Volume One Trauma 2017Fawzia Haznah Nurul Imani100% (8)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Critical Care AnesthesiaDocument451 pagesCritical Care AnesthesiaMichael Andrews100% (7)
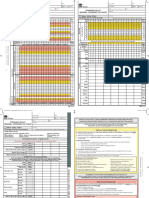
- SAGO AdultObsDocument2 pagesSAGO AdultObsTim BrownNo ratings yet
- Neonatal SepsisDocument29 pagesNeonatal SepsisElton Ndhlovu100% (3)
- Research-Food and Nutrition Research - Microbial Analysis On Utensils PDFDocument46 pagesResearch-Food and Nutrition Research - Microbial Analysis On Utensils PDFZenaida BonifacioNo ratings yet
- DO /VO Relationships: J. L. VincentDocument8 pagesDO /VO Relationships: J. L. VincentLucas Cárcamo SaavedraNo ratings yet
- Drug Used in The Therapy of Shock.Document8 pagesDrug Used in The Therapy of Shock.Vennela100% (1)
- MCQ Maret 2021Document16 pagesMCQ Maret 2021promkes poloNo ratings yet
- Pneumonia: Pneumonia Is An Inflammatory Condition of The Lung. It Is Often Characterized AsDocument13 pagesPneumonia: Pneumonia Is An Inflammatory Condition of The Lung. It Is Often Characterized AsBettina Gem M. PeñalosaNo ratings yet
- Test Bank Chapter 67: Nursing Management: Shock, Systemic Inflammatory Response Syndrome, and Multiple Organ Dysfunction SyndromeDocument11 pagesTest Bank Chapter 67: Nursing Management: Shock, Systemic Inflammatory Response Syndrome, and Multiple Organ Dysfunction Syndromebbianca1990100% (1)
- Sepsis Guidelines 2012Document13 pagesSepsis Guidelines 2012Lauren WilkersonNo ratings yet
- Annalsats Articles in Press. Published February 03, 2023 As 10.1513/Annalsats.202211-946OcDocument33 pagesAnnalsats Articles in Press. Published February 03, 2023 As 10.1513/Annalsats.202211-946OcAlexandre Cavalcanti100% (1)
- Antibiotik StewardshipDocument13 pagesAntibiotik StewardshipSeptiandry Ade PutraNo ratings yet
- Clinical Review: Blood Purifi Cation For SepsisDocument10 pagesClinical Review: Blood Purifi Cation For SepsisVlady78No ratings yet
- Separations: Extraction, Quantification, and Cytokine Inhibitory Response of Bakuchiol in Psoralea Coryfolia LinnDocument11 pagesSeparations: Extraction, Quantification, and Cytokine Inhibitory Response of Bakuchiol in Psoralea Coryfolia LinnKandida Hilda NovikaNo ratings yet
- Neonatal SepsisDocument6 pagesNeonatal SepsisSunaina AdhikariNo ratings yet
- Effect of Emollient Therapy On Clinical Outcomes PDFDocument7 pagesEffect of Emollient Therapy On Clinical Outcomes PDFYESSICA MARCELA RODRIGUEZ QUECHONo ratings yet
- Antipyretic Therapy in Critically Ill Septic Patients - A Systematic Review and Meta-AnalysisDocument8 pagesAntipyretic Therapy in Critically Ill Septic Patients - A Systematic Review and Meta-AnalysisKrutarth PatelNo ratings yet
- Methylene Blue: Revisited: Clinical PharmacologyDocument4 pagesMethylene Blue: Revisited: Clinical PharmacologyMahtosurup GodavarthyNo ratings yet
- Nursing Care Plan On SepsisDocument6 pagesNursing Care Plan On SepsisleoNo ratings yet
- Leptospirosis: A Case Study: Mathew SullivanDocument3 pagesLeptospirosis: A Case Study: Mathew SullivanSagara MaheshNo ratings yet
- Manejo de CoagulopatiaDocument4 pagesManejo de CoagulopatiaSMIBA MedicinaNo ratings yet
- Final General Surgery (1) - 230122 - 192353Document49 pagesFinal General Surgery (1) - 230122 - 192353Lika BukhaidzeNo ratings yet
- Why We Need A New Definition of Sepsis: Sarah J. Beesley, Michael J. LanspaDocument4 pagesWhy We Need A New Definition of Sepsis: Sarah J. Beesley, Michael J. LanspaOana MariaNo ratings yet
- Materi Bu CostiDocument36 pagesMateri Bu CostitriaNo ratings yet
- Septic Shock: Dr. Dr. Hori Hariyanto, Span, Kic, KMNDocument89 pagesSeptic Shock: Dr. Dr. Hori Hariyanto, Span, Kic, KMNPander MadonNo ratings yet
- Atb NeosDocument13 pagesAtb NeosAnonymous 44bTHDeHkbNo ratings yet
- Neonatal Sepsis: Assessment and CareDocument51 pagesNeonatal Sepsis: Assessment and CareParbatiNo ratings yet
- Common Surgical ProblemsDocument20 pagesCommon Surgical ProblemsSasha KhomaNo ratings yet
- Continous Renal Replacement Therapy Principles, Modalities, and PrescribtionDocument9 pagesContinous Renal Replacement Therapy Principles, Modalities, and PrescribtionhendramcpheeNo ratings yet