Professional Documents
Culture Documents
Comparison of MERGE and Axial T2-Weighted Fast Spin-Echo Sequences For Detection of Multiple Sclerosis Lesions in The Cervical Spinal Cord
Uploaded by
Otong Zam ZamyOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Comparison of MERGE and Axial T2-Weighted Fast Spin-Echo Sequences For Detection of Multiple Sclerosis Lesions in The Cervical Spinal Cord
Uploaded by
Otong Zam ZamyCopyright:
Available Formats
Neuroradiolog y / Head and Neck Imaging Original Research
Martin et al.
MRI Detection of Multiple Sclerosis
Neuroradiology/Head and Neck Imaging
Original Research
Comparison of MERGE and Axial
T2-Weighted Fast Spin-Echo
Downloaded from www.ajronline.org by 36.82.102.157 on 03/04/17 from IP address 36.82.102.157. Copyright ARRS. For personal use only; all rights reserved
Sequences for Detection of
Multiple Sclerosis Lesions in
the Cervical Spinal Cord
Nancy Martin1 OBJECTIVE. The purpose of our study was to compare axial multiple-echo recombined
David Malfair 2 gradient echo (MERGE) with axial T2-weighted fast spin-echo (FSE) imaging for the de-
Yinshan Zhao 3 tection of multiple sclerosis (MS) lesions in the cervical spinal cord on MRI.
David Li1 MATERIALS AND METHODS. Twenty-nine cervical spine MRI studies of patients
Anthony Traboulsee 3 with MS lesions and 29 control cases were reviewed retrospectively. Two blinded neuroradi-
ologists independently assessed randomized axial MERGE and axial T2-weighted FSE se-
Donna Lang 4
quences from each study, documenting the location and number of cord lesions, the degree of
Alexandra Talia Vertinsky 1 confidence in calling each lesion, and the presence of artifacts. The reference standard was
Martin N, Malfair D, Zhao Y, et al. determined by an unblinded consensus review of all sequences performed for each case, with
lesions considered present if detected on two or more sequences. Lesion detection rates and
conspicuity, false-positive findings, and reader confidence and artifact scores were compared
for the sequences, and interreader agreement was assessed.
RESULTS. Eighty-three lesions were assessed. The mean true-positive lesion detection
rate was 87% (95% CI, 7993%) with MERGE and 67% (6075%) with T2-weighted FSE,
with interreader positive agreement scores of 74% and 75%, respectively. A greater number
of false-positive findings were seen with MERGE for both the MS and control cases. Aver-
age confidence and artifact scores were similar for both sequences. Subjectively, lesions were
more conspicuous in 21 cases with MERGE and four cases with T2-weighted FSE and were
equally conspicuous in four cases.
CONCLUSION. MERGE and T2-weighted FSE sequences are complementary.
MERGE provided greater sensitivity for cord lesions whereas axial T2-weighted FSE provid-
ed improved lesion specificity. Further investigation is required to assess the clinical impact
Keywords: MRI, multiple sclerosis, spinal cord of MERGE in the diagnosis and management of MS.
DOI:10.2214/AJR.11.7039
C
ervical spine MRI is important in intermediate uveitis) and ischemic processes.
Received April 14, 2011; accepted after revision the workup of demyelinating dis- The presence of spinal cord lesions, however,
November 13, 2011.
ease, particularly suspected mul- is more specific to MS, with the presence of a
1
Department of Radiology, University of British Columbia
tiple sclerosis (MS). Spinal cord cord abnormality alone providing up to 92%
Hospital, 2211 Westbrook Mall, Vancouver, BC, Canada abnormalities are seen on MRI in up to 83% of accuracy in identifying MS among other neu-
V6T 2B5. Address correspondence to N. Martin newly diagnosed MS patients [1] and support rologic disorders [2].
(nmtmartin@gmail.com). an atypical clinical presentation or equivocal Spinal cord abnormalities seen on MRI were
2 brain MRI by ruling out alternative pathology formally incorporated into the McDonald di-
Red Deer Regional Hospital, Red Deer, AB, Canada.
and improving imaging sensitivity and speci- agnostic criteria for MS in 2005 [3]. The cur-
3
Department of Medicine, Division of Neurology, ficity. Bot et al. [1] showed that the inclusion rent recommendations for spinal cord imaging
University of British Columbia Hospital, Vancouver, BC, of a single spinal cord lesion in addition to include axial and sagittal T2-weighted, sagittal
Canada. brain imaging findings allowed 84.6% of new- T1-weighted, and sagittal STIR or proton den-
4
Department of Radiology, CFRI BCMHARI Centre for
ly diagnosed MS patients to meet the McDon- sity sequences, with the option for additional
Complex Disorders, BC Childrens Hospital, Vancouver, ald criteria for dissemination of disease in contrast-enhanced T1-weighted imaging for
BC, Canada. space, compared with only 66.3% using brain suspicious lesions and 3D inversion recovery
imaging alone. White matter lesions detected prepared T1 gradient-echo sequences [4]. De-
AJR 2012; 199:157162 in the brain by MRI are often nonspecific, with spite advances in cardiac gating and phased-
0361803X/12/1991157
significant overlap between MS and many oth- array coils, spatial and contrast resolution and
er CNS inflammatory (e.g., systemic lupus er- motion and pulsation artifact remain limiting
American Roentgen Ray Society ythematosus, sarcoidosis, Sjgren syndrome, factors in current protocol acquisitions.
AJR:199, July 2012 157
Martin et al.
A number of sequences have been stud- lent bone-CSF-soft tissue contrast [11, 13, 14], weighted (TR range/TE range, 30003500/102
ied in an attempt to improve spinal cord le- and option of 3D acquisition. MERGE, howev- 110; echo-train length, 1523; bandwidth, 1631
sion detection. The FLAIR sequence, despite er, also shows excellent gray-white matter res- kHz; matrix, 256320 256; slice thickness, 3
superior lesion detection in the supratentori- olution (Fig. 1), making it ideal for assessment mm; 0.5- to 1-mm skip; FOV, 20 cm; and num-
al brain, does not perform well in the spinal of intramedullary pathology [11, 13]. A small ber of signals acquired, 4), axial T2-weighted FSE
cord because it is hampered by CSF pulsa- study comparing MEDIC with magnetization (TR range/TE range, 28003250/102110; echo-
Downloaded from www.ajronline.org by 36.82.102.157 on 03/04/17 from IP address 36.82.102.157. Copyright ARRS. For personal use only; all rights reserved
tion artifact, poor contrast-to-noise ratio, and transfer to standard T2-weighted turbo spin- train length, 1526; bandwidth, 1631 kHz; ma-
poor lesion detection [5]. Although STIR has echo, STIR, and T1 spin-echo unenhanced and trix, 256 224 slice thickness, 3 mm; 1-mm skip;
shown improved lesion detection and conspi- contrast-enhanced sequences has shown superi- FOV, 20 cm; and number of signals acquired, 4),
cuity over T2-weighted fast spin-echo (FSE) or visibility of intramedullary hemorrhage and and axial MERGE (TR range, 9501000; band-
and T2-weighted conventional spin-echo im- mild cord edema as well as improved contrast width, 31 kHz; matrix, 288 192; slice thickness,
aging [58], poor signal-to-noise ratio (SNR) between spinal cord gray matter, white matter, 3 mm; 1-mm skip; FOV, 20 cm; and number of
[5, 8, 9], interpretative limitations due to flow and edema on MEDIC [15]. To date, however, signals acquired, 2). A variable number of addi-
and motion artifacts, and poor interobserv- there have been no studies comparing MERGE tional sequences were performed in each case, in-
er agreement [10] have also been described. to standard sequences in the MRI workup of cluding sagittal T1-weighted, sagittal STIR, and
Standard gradient-echo imaging has shown MS. In this article, we compare the ability of sagittal or axial proton densityweighted.
improved lesion detection over T2-weighted MERGE and axial T2-weighted FSE to detect
FSE when used with magnetization transfer focal T2-hyperintense lesions in the cervical Image Evaluation
[6] but has limited gray-white matter contrast spinal cord. The MERGE and axial T2-weighted FSE se-
[11]. More recently, T1-weighted inversion quences from both healthy and MS patients were ran-
recovery has shown promise, with improved Materials and Methods domized and presented separately on workstations
contrast between demyelinating lesions and Case Selection for independent review by two neuroradiologists who
normal cervical cord relative to T2-weighted The study was approved by the institutional clin- were blinded to the clinical information. For each se-
FSE and STIR as well as improved lesion lo- ical ethics research board. Our institutional data- quence, the reviewers documented the location of any
calization and delineation, particularly with base was searched from January 2005 to Decem- cord lesions, assigned a confidence score in calling
phase-sensitive reconstruction [12], but has ber 2008 for cervical spine MRI cases reported to each lesion (from 1 indicating low confident to 5 in-
not yet been widely implemented. have focal spinal cord lesions consistent with MS. dicating high confidence), and assigned an overall se-
There is a relatively new gradient-echo se- Patients were included if they had focal T2-hyper- quence artifact score to each series of images (from 1
quence that combines multiple bipolar gradi- intense lesions and if at least sagittal and axial T2- indicating severe to 5 indicating none). After comple-
ent-echo formations using early echoes to in- weighted FSE and axial MERGE sequences were tion of the independent reviews, the reference stan-
crease SNR and later echoes to increase image performed as part of a standard clinical imaging dard of spinal cord lesions was determined by an un-
contrast. This sequence is known by a variety protocol. Control cases were identified in a similar blinded consensus review of the MS cases by one
of acronyms depending on the equipment ven- fashion by searching the institutional database for of the neuroradiologists and a third radiologist with
dor: MERGE (multiple-echo recombined gra- cases performed for indications other than MS and experience in neurologic MRI. Spinal cord lesions
dient echo) for GE Healthcare, MEDIC (mul- in whom the spinal cord was reported as normal. were considered present if visible on two or more of
tiecho data image combination) for Siemens Only the 29 most recent control subjects were se- the available sequences in a given case. In review of
Healthcare, and MFFE (multiecho fast field lected to match the number of MS cases. each case during the consensus review, MERGE and
echo) for Philips Healthcare. To date, this se- T2-weighted FSE were also directly compared side-
quence has most commonly been used to re- MRI Parameters by-side for overall lesion conspicuity, and the false-
place the standard T2* gradient-echo sequence The studies were acquired on one of two 1.5-T positive lesions among the control subjects were in-
for assessment of disk pathology in the cervical systems (Signa, GE Healthcare) with a phased-ar- dividually examined for characterization. One of the
spine [11], benefitting from its reduced pulsa- ray head, neck, and spine coil using a standardized MS cases was rejected during the consensus review
tion artifact relative to T2-weighted FSE, excel- clinical protocol that included sagittal FSE T2- because of severe patient motion artifact affecting all
sequences and significantly limiting assessment.
Statistical Analysis
The number of lesions identified independent-
ly by a given reader using MERGE and axial T2-
weighted FSE sequences in isolation were com-
pared with each other and to the reference lesion
Fig. 134-year-old woman with left-sided
radiculopathy (normal control group).
A, Axial multiple-echo recombined gradient echo
(MERGE) image shows excellent gray-white matter
differentiation in cervical spinal cord.
B, Axial T2-weighted fast spin-echo image through
same level as A shown for comparison.
A B
158 AJR:199, July 2012
MRI Detection of Multiple Sclerosis
TABLE 1: Lesion Counts in Multiple Sclerosis Cases
MERGE T2-Weighted FSE
Parameter Reader 1 Reader 2 Reader 1 Reader 2
True-positive lesions 67 78 58 53
Reference true-positive lesions) (%)a 81 94 70 64
Downloaded from www.ajronline.org by 36.82.102.157 on 03/04/17 from IP address 36.82.102.157. Copyright ARRS. For personal use only; all rights reserved
95% CI (%) 6990 8998 5980 5575
False-positive lesions 20 21 10 7
Total lesions 87 99 68 60
NoteMERGE = multiple-echo recombined gradient echo, FSE = fast spin-echo.
a Also referred to as true-positive detection rate or sensitivity.
count using the Wilcoxon signed rank test. Sequence dent case review were significantly higher with the potential for misclassifying six cas-
sensitivities for true-positive lesions were calcu- with MERGE compared with T2-weighted es as possible MS for both sequences. Al-
lated, with 95% CIs obtained for each reading us- FSE: 28% higher for reader 1 (p = 0.01) and though false-positive counts in the control
ing the cluster bootstrapping method [16] and each 65% higher for reader 2 (p = 0.0007). cases were higher using MERGE, the differ-
subject as a sampling unit. The sensitivities of the After comparison with the reference stan- ence did not reach statistical significance (p =
two readings from the same reader were compared dard, the sensitivity for true-positive lesions, 0.27 for reader 1 and p = 0.36 for reader 2).
using the two-sided Mosteller exact test [17]. or the true-positive detection rate, was also The false-positive lesions seen with MERGE
The mean confidence scores assigned to lesions higher using MERGEsignificantly so for in the control cases were attributable to mo-
by the same reader were compared using the z score, reader 2 (p < 0.05) but not for reader 1 (p = tion artifact (7/23 lesions), poor SNR (4/23),
with MS and control cases analyzed separately. The 0.06) (Table 1). The mean true-positive lesion blurring of the gray matter (9/23), and misin-
standard error of the mean difference of these scores detection rate for both readers was 87% (95% terpretation of prominent gray matter signal
was obtained using cluster bootstrapping. We first CI, 7993%) for MERGE and 67% (6075%) and the central canal in the high cervical cord
compared the scores for all lesions called by a giv- for T2-weighted FSE. Although total lesion (3/23). Of note, susceptibility artifact did
en reader, then for the true-positive and false-pos- counts and the true-positive detection rate var- not impact cord signal and was not a source
itive lesions separately. Because of small lesion ied significantly between the two readers us- of false-positive findings with MERGE. As
counts, p values were not calculated for the false- ing MERGE but not using T2-weighted FSE, for T2-weighted FSE, false-positive lesions
positive lesions among the control groups. lesion-by-lesion true-positive interreader per- were related to CSF pulsation artifact (4/9),
The interreader agreement was measured by the centage positive agreement was similar for poor signal to noise (4/9), and blurring of the
percentage of positive agreement index [18]. This both sequences: 74% for MERGE and 75% white matter (1/9).
index reflects the chance that if one reader identi- for T2-weighted FSE. False-positive lesion The mean confidence scores assigned to
fied a site as a lesion, another reader will also iden- counts for the MS patients were significantly all lesions are summarized in Table 2. Con-
tify the same site. Under perfect agreement, the higher with MERGE relative to T2-weighted fidence scores ranged from 2 to 5, with a low
probability is 1. Standard errors and CIs were ob- FSE for both readers (p = 0.05) (Table 1). confidence score of 2 being assigned only
tained using the bootstrapping method. Sequence False-positive lesions were also called in twice: once to a false-positive lesion within
artifact scores assigned by the same reader were the control cases using both sequences. Read- a control case and the other to a true-positive
compared using the Wilcoxon signed rank test. er 1 called a total of eight false-positive le- lesionboth cases using T2-weighted FSE.
sions using MERGE compared with two us- Except for reader 2, who had higher confi-
Results ing T2-weighted FSE, which could have dence scores for true-positive lesions with the
The consensus review identified 83 refer- mistakenly classified four cases and one case MERGE sequence, mean confidence scores
ence-standard lesions among the MS cases. as potential MS, respectively. For reader 2, did not differ significantly between sequenc-
The total number of lesions (both true- and 16 false-positive lesions were called using es. There was, however, suggestion of a trend
false-positive) identified during the indepen- MERGE and eight using T2-weighted FSE, toward progressively lower confidence scores
TABLE 2: Lesion Confidence Scores
Reader 1 Reader 2
Parameter MERGE T2-Weighted FSE p MERGE T2-Weighted FSE p
Mean confidence score per lesiona 4.56 4.68 0.39 4.71 4.55 0.24
Mean confidence score per true-positive lesion 4.67 4.72 0.70 4.87 4.60 0.02
Mean confidence score per false-positive lesion in MS cases 4.20 4.40 0.54 4.10 4.14 0.92
Mean confidence score per false-positive lesion in control cases 3.50 3.00 NA 3.59 2.83 NA
NoteConfidence was scored on 5-point scale from 1 (lowest) to 5 (highest), degree of confidence in calling each lesion. Because of insufficient counts, p values were
not calculated for the control cases. MERGE = multiple-echo recombined gradient echo, FSE = fast spin-echo, MS = multiple sclerosis, NA = not applicable.
aBoth true-positive and false-positive lesions called by a given reader.
AJR:199, July 2012 159
Martin et al.
Fig. 228-year-old man with relapsing remitting
multiple sclerosis.
A, Axial multiple-echo recombined gradient echo
(MERGE) image shows small lesion abuts right
posterior horn (arrow). Although lesion is small,
because posterior horn is well defined (normal
appearance one slice below as shown in C), discrete
lesion can be confidently called.
Downloaded from www.ajronline.org by 36.82.102.157 on 03/04/17 from IP address 36.82.102.157. Copyright ARRS. For personal use only; all rights reserved
B, At same level as A, only subtle ill-defined focus of
increased signal is seen on axial T2-weighted fast
spin-echo (FSE) image in region of right posterior
horn (arrow), which may be interpreted as part of
normal gray matter, if appreciated at all.
C, On axial MERGE image, focal lesion within
posterior central cervical cord (arrow) is easily
identified.
D, Axial T2-weighted FSE image at same level as C
A B shows posterior white matter lesion is very subtle.
Lesion was only appreciated in retrospect on axial
T2-weighted FSE images.
weaknesses for identifying MS lesions have
not been characterized.
In our study, MERGE showed improved
sensitivity for the detection of spinal cord le-
sions, with more true-positive lesions than
T2-weighted FSE (Fig. 3). One reason for
the higher true-positive lesion detection is
the improved anatomic depiction of the nor-
mal H-shaped bright central gray matter on a
background of low-signal white matter (Fig.
C D 1), which permits improved distinction of
pathologic high-signal foci. When the gray-
assigned in the descending order of true-posi- pulsation artifact was documented on 43 and white boundary is less well defined, patho-
tive lesions, false-positive lesions in MS cas- motion on nine of the 116 T2-weighted FSE logic signal change not completely in the pe-
es, and false-positive lesions in control cases. scoring sheets. Although the low numbers riphery of the cord may be confused with
Subjectively, when the sequences were com- and lack of standardized documenting limit normal central gray matter (Figs. 2A and
pared side by side during the consensus re- the analysis of this information, MERGE was 2B). The increased conspicuity of lesions
view, lesions were more conspicuous in 21 also found to be more easily degraded by pa- on MERGE relative to T2-weighted FSE in
cases (72%) with MERGE (Fig. 2) and four tient motion when directly compared with T2- 72% of cases also likely contributed to this
cases with T2-weighted FSE and were equally weighted FSE during the consensus review. increased sensitivity (Figs. 2C and 2D).
conspicuous in four cases. CSF pulsation artifact was documented on Although one might have expected the
Averaged for both readers, the arti- more than one third of the T2-weighted FSE confidence scores in calling a lesion to reflect
fact scores (SD) were 3.93 ( 0.73) for the scoring sheets and was responsible for almost lesion conspicuity, our subjective assessment
MS patients and 3.64 ( 0.88) for the con- one half of the false-positive lesions in the that cord lesions were more conspicuous on
trol subjects with MERGE compared with control subjects with T2-weighted FSE (as de- MERGE did not translate into higher confi-
3.89 (0.53) for the MS patients and 3.78 ( scribed earlier); however, an artifact score of dence ratings. This is explained, at least in
0.51) for the control subjects with T2-weight- less than 3 was never assigned when pulsation part, by the fact that confidence scores be-
ed FSE. Although average artifact scores were artifact alone was documented. low 3 were almost never assigned; a lesion
similar between the two sequences, the artifact was unlikely to be called if confidence was
scores assigned to MERGE were more vari- Discussion low. In that light, improved lesion conspicu-
able, with a higher proportion of lower (1 and Evaluation of the spinal cord with MRI is ity with MERGE has not been reflected on a
2) and high (5) scores. The readers were not challenging because of the small size of the lesion-by-lesion basis but rather by improved
required to document the types of artifacts on spinal cord, CSF pulsation artifact, and sus- sensitivity for detecting an increased number
their scoring sheets; however, both readers did ceptibility and ringing artifacts from the prox- of lesions conspicuous enough to prospec-
make occasional notes on the types of artifact imity of the bony spinal canal. Many sequenc- tively call with confidence.
present during their independent reviews. In- es have been studied in an attempt to optimize At the expense of higher lesion detection
cluding the scoring sheets from both readers spinal cord lesion detection. MERGE is a rela- with MERGE is a higher number of false-
and for both the control and MS cases, motion tively new sequence with excellent gray-white positive findings and the potential misclassi-
was documented on 21 of the 116 MERGE matter contrast that has shown promise in fication of normal control cases as MS cases.
scoring sheets. No other specific artifact was identifying edema and hemorrhage within the Some of these lesions may simply have not
mentioned for MERGE. In comparison, CSF cervical spinal cord [15], but its strengths and been shown well enough on the non-MERGE
160 AJR:199, July 2012
MRI Detection of Multiple Sclerosis
against lesions seen only on the single axi-
al MERGE sequence. Additionally, the ret-
rospective review of axial sequences in iso-
lation is artificial and limits our ability to
translate the differences in sensitivity and
specificity of MERGE and T2-weighted FSE
Downloaded from www.ajronline.org by 36.82.102.157 on 03/04/17 from IP address 36.82.102.157. Copyright ARRS. For personal use only; all rights reserved
into the setting of a complete imaging proto-
col and clinical practice.
Conclusion
This head-to-head comparison of axial
MERGE and axial T2-weighted FSE sequenc-
es has shown these sequences to be comple-
A B mentary, each providing unique advantages in
Fig. 342-year-old woman with multiple sclerosis who presented with progressive lower limb spasticity. the identification of MS lesions. The superi-
A, Axial multiple-echo recombined gradient echo (MERGE) image shows right posterolateral (white arrow) and or gray-white matter differentiation within the
posterior central (black arrow) lesions within high cervical cord. spinal cord and the increased contrast and con-
B, No convincing abnormality is seen at corresponding level on axial T2-weighted fast spin-echo image,
representing two false-negative lesions: right posterolateral (white arrow) and posterior central (black arrow)
spicuity of cord lesions with MERGE relative
lesions. to T2-weighted FSE allow improved detection
of intramedullary lesions but at the price of a
sequences to be included in the reference an additional lesion that individually may be higher false-positive rate. Thus, although ax-
standard. Because the sagittal T2-weighted less conspicuous. Thus, lesions with a ques- ial T2-weighted FSE has greater specificity,
FSE sequence was one of the main sequenc- tionable appearance, requiring correlation MERGE shows greater sensitivity, suggesting
es used to confirm lesions present in the axial with other sequences, received lower con- the two sequences together have the potential
plane, bias may have been introduced to cat- fidence scores, whereas the presence or ab- to improve the workup of patients with sus-
egorize lesions detected on T2-weighted FSE sence of additional cord lesions further strati- pected MS. Further investigations are warrant-
as true-positive lesions and those on MERGE fied the false-positive lesions among MS and ed to assess the impact of including MERGE
as false-positive lesions. However, the pres- control cases, respectively. In practice, ques- in current imaging protocols in meeting di-
ence of increased false-positive lesions on tionable lesions seen on one sequence would agnostic criteria for MS and changing subse-
MERGE within the control cases indicates be correlated with additional sequences for quent clinical management.
that overcalls do occur and will be a limitation confirmation or rejection, reducing the false-
of MERGE if viewed independently. Anoth- positive rate of both sequences. References
er possible reason for the higher false-posi- Degradation of images by patient mo- 1. Bot JC, Barkhof F, Polman CH, et al. Spinal cord
tive rate with MERGE is the lack of familiari- tion was the main source of artifacts in the abnormalities in recently diagnosed MS patients:
ty with this sequence compared with standard MERGE images and a significant source of added value of spinal MRI examination. Neurol-
T2-weighted FSE. Greater clinical experience false-positive lesions called with MERGE in ogy 2004; 62:226233
with MERGE may translate into improved the control cases. Although MERGE shows 2. Bot JC, Barkhof F, Nijeholt G, et al. Differentia-
specificity and confidence in assessment of excellent gray-white matter differentiation tion of multiple sclerosis from other inflammatory
spinal cord lesions with MERGE over time. under ideal circumstances, when motion ar- disorders and cerebrovascular disease: value of
Although confidence scores did not dif- tifact is present, there is substantial blurring spinal MR imaging. Radiology 2002; 223:4656
fer significantly between sequences, they did of the bright central gray matter. This motion 3. Polman CH, Reingold SC, Edan G, et al. Diagnos-
reveal an interesting trend of progressively artifact may be a reason for decreased spec- tic criteria for multiple sclerosis: 2005 revisions to
lower confidence scores assigned in descend- ificity in some cases and may also explain the McDonald Criteria. Ann Neurol 2005; 58:
ing order of true-positive lesions, false-posi- the variability of the artifact scores assigned 840846
tive lesions among the MS cases, and false- to MERGE. In comparison, the decreased 4. Li D, Stone L, Harper J, et al. Consortium of Mul-
positive lesions among the control cases. variability of artifact scores assigned to T2- tiple Sclerosis Centers (CMSC) guidelines for a
Lower confidence scores among the false- weighted FSE suggests the presence of CSF standardized MRI protocol for the diagnosis and
positive lesions most likely reflect simply a pulsation artifactdespite being present in follow-up of multiple sclerosis: 2009 revision. J
questionable imaging appearance, either due more than one third of cases and accounting Neurol Sci 2009; 285(suppl 1):S78S79
to decreased conspicuity of an individual le- for one half of the control case false-positive 5. Hittmair K, Mallek R, Prayer D, et al. Spinal cord
sion or suspicion that the finding represents lesionshas less impact on cord evaluation lesions in patients with multiple sclerosis: com-
artifact or even normal anatomy. than motion does when using MERGE. parison of MR pulse sequences. AJNR 1996;
Although confidence scores were assigned Our study has several limitations. First, 17:15551565
on a per-lesion basis, this subjective assess- our reference standard consisted of a review 6. Rocca MA, Mastronardo G, Horsfield MA, et al.
ment is influenced not only by their appear- of all sequences performed rather than path- Comparison of three MR sequences for the detec-
ance but also by the presence or absence of ologic confirmation. The presence of both tion of cervical cord lesions in patients with mul-
lesions at other levels. The presence of multi- axial and sagittal T2-weighted FSE sequenc- tiple sclerosis. AJNR 1999; 20:17101716
ple lesions will increase confidence in calling es, but only axial MERGE, introduces a bias 7. Campi A, Pontesilli S, Gerevini S, Scotti G. Com-
AJR:199, July 2012 161
Martin et al.
parison of MRI pulse sequences for investigation 11. Vertinsky AT, Krasnokutsky MV, Augustin M, et sequence with a magnetisation transfer saturation
of lesions of the cervical spinal cord. Neuroradi- al. Cutting edge imaging of the spine. Neuroimag- pulse and cervical myelography and CT. Neurora-
ology 2000; 42:669675 ing Clin N Am 2007; 17:117136 diology 2004; 46:306309
8. Mascalchi M, Dal Pozzo G, Bartolozzi C. Effec- 12. Poonawalla AH, Hou P, Nelson FA, et al. Cervical 15. Held P, Dorenbeck U, Seitz J, et al. MRI of the ab-
tiveness of the short TI inversion recovery (STIR) spinal cord lesions in multiple sclerosis: T1- normal cervical spinal cord using 2D spoiled gradi-
sequence in the MR imaging of intramedullary spi- weighted inversion-recovery MR imaging with ent echo multiecho sequence (MEDIC) with mag-
Downloaded from www.ajronline.org by 36.82.102.157 on 03/04/17 from IP address 36.82.102.157. Copyright ARRS. For personal use only; all rights reserved
nal lesions. Magn Reson Imaging 1993; 11:1725 phase-sensitive reconstruction. Radiology 2008; netization transfer saturation pulse: a T2* weighted
9. Thorpe JW, MacManus DG, Kendall BE, et al. 246:258264 feasibility study. J Neuroradiol 2003; 30:8390
Short tau inversion recovery fast spin-echo (fast 13. Held P, Seitz J, Frund R, et al. Comparison of two- 16. Davison AC, Hinkley DV. Bootstrap methods and
STIR) imaging of the spinal cord in multiple scle- dimensional gradient echo, turbo spin echo and their application. Cambridge, United Kingdom:
rosis. Magn Reson Imaging 1994; 12:983989 two-dimensional turbo gradient spin echo se- Cambridge University Press, 1997:101104
10. Bot JC, Barkhof F, Lycklama a Nijeholt GJ, et al. quences in MRI of the cervical spinal cord anato- 17. Agresti A. Categorical data analysis, 2nd ed.
Comparison of a conventional cardiac-triggered my. Eur J Radiol 2001; 38:6471 Hoboken, NJ: John Wiley & Sons, 2002:347352
dual spin-echo and a fast STIR sequence in detec- 14. Dorenbeck U, Schreyer AG, Schlair J, et al. De- 18. Cicchetti DV, Feinstein AR. High agreement but
tion of spinal cord lesions in multiple sclerosis. generative diseases of the cervical spine: com- low kappa. Part II. Resolving the paradoxes. J
Eur Radiol 2000; 10:753758 parison of a multiecho data image combination Clin Epidemiol 1990; 43:551558
F O R YO U R I N F O R M AT I O N
Unique customized medical search engine service from ARRS! ARRS GoldMiner is a keyword- and
concept-driven search engine that provides instant access to radiologic images published in peer-reviewed
journals. For more information, visit http://goldminer.arrs.org.
162 AJR:199, July 2012
You might also like
- Interpretting ABG SuccessfullyDocument15 pagesInterpretting ABG Successfullyanimathz100% (1)
- Total Leukocyte Count by HemocytometerDocument4 pagesTotal Leukocyte Count by HemocytometerMalkish RajkumarNo ratings yet
- Approach To MRI Management in Stroke - PARI Kota MakassarDocument50 pagesApproach To MRI Management in Stroke - PARI Kota MakassarASMARNo ratings yet
- 2.3. Mental Health Nursing: Course DescriptionDocument5 pages2.3. Mental Health Nursing: Course Descriptioncharanjit kaurNo ratings yet
- Nursing Care Plan - Pericarditis PatientDocument2 pagesNursing Care Plan - Pericarditis Patientsandie_best78% (9)
- Typhoid Fever NCPDocument46 pagesTyphoid Fever NCPLyra Lustre RN67% (3)
- 2022 Book AntimicrobialResistanceDocument606 pages2022 Book AntimicrobialResistanceFety Andriani100% (1)
- MRI Monitoring of Pathological Changes in The Spinal Cord in Patients With Multiple SclerosisDocument13 pagesMRI Monitoring of Pathological Changes in The Spinal Cord in Patients With Multiple SclerosisIreneNo ratings yet
- Fnana 2010 00015 PDFDocument7 pagesFnana 2010 00015 PDFROHITNo ratings yet
- Comparison ofDocument10 pagesComparison ofTecnologos 4º turnoNo ratings yet
- Foci Signal (Pseudo Lesions) To The Frontal: of Mri Anterior HornsDocument7 pagesFoci Signal (Pseudo Lesions) To The Frontal: of Mri Anterior HornsNourhan AliNo ratings yet
- Intrarater and Interrater Reliability of Quantitative Thigh Muscle Magnetic Resonance ImagingDocument10 pagesIntrarater and Interrater Reliability of Quantitative Thigh Muscle Magnetic Resonance ImagingEdgarNo ratings yet
- Monitoring dermatomal somatosensory evoked potentials at multiple levelsDocument8 pagesMonitoring dermatomal somatosensory evoked potentials at multiple levelsStephii AguirreNo ratings yet
- Electrodiagnosis in Spinal Disorders - Spine SecretsDocument9 pagesElectrodiagnosis in Spinal Disorders - Spine SecretsPaulina Chinchilla LópezNo ratings yet
- neckshaft angleDocument5 pagesneckshaft angleritee.shresthaNo ratings yet
- Ajr 2Document3 pagesAjr 2anon_302681452No ratings yet
- cVEMP y oVEMP en ESCLEROSIS MULTIPLEDocument8 pagescVEMP y oVEMP en ESCLEROSIS MULTIPLEJaneth GuzmanNo ratings yet
- J Neulet 2010 03 029Document4 pagesJ Neulet 2010 03 029Andres Rojas JerezNo ratings yet
- 1 s2.0 S1878875019327561 MainDocument21 pages1 s2.0 S1878875019327561 MainandresNo ratings yet
- Horger Et Al 2012 Imaging Findings in Tick Borne Encephalitis With Differential Diagnostic ConsiderationsDocument8 pagesHorger Et Al 2012 Imaging Findings in Tick Borne Encephalitis With Differential Diagnostic ConsiderationsNeurobites ESLNo ratings yet
- Using MRI To Characterize Pedicle Asymmetry in SPINEDocument8 pagesUsing MRI To Characterize Pedicle Asymmetry in SPINER BNo ratings yet
- Seguridad Social en AlemaniaDocument8 pagesSeguridad Social en AlemaniaMichael RojasNo ratings yet
- Ajr.09.2772 Grading Neuroforaminal StenosisDocument4 pagesAjr.09.2772 Grading Neuroforaminal StenosisOscar NogueraNo ratings yet
- Ligaments of The Transverse Tarsal Joint Complex: MRI-Anatomic Correlation in CadaversDocument10 pagesLigaments of The Transverse Tarsal Joint Complex: MRI-Anatomic Correlation in CadaversSaifuddin HaswareNo ratings yet
- High Contrast High Resolution Imaging of PosttraumDocument10 pagesHigh Contrast High Resolution Imaging of PosttraumPaulo Ferreira OrtodontiaNo ratings yet
- Differences in Neural Connectivity Between The SubstantiaDocument5 pagesDifferences in Neural Connectivity Between The SubstantiaPamGarcíaNo ratings yet
- Combined Eeg and Mri Studies of Human Brain Function: V. Menon and S. Crottaz-HerbetteDocument31 pagesCombined Eeg and Mri Studies of Human Brain Function: V. Menon and S. Crottaz-HerbetteShalini VijayNo ratings yet
- Motor Nerve To The Vastus LateralisDocument4 pagesMotor Nerve To The Vastus LateralisIsaac SamuelNo ratings yet
- A Technique For Studying The Greater Auricular Nerve Conduction VelocityDocument3 pagesA Technique For Studying The Greater Auricular Nerve Conduction Velocityfernando gonzalezNo ratings yet
- 21436-Vascular Anatomy - VilelaDocument12 pages21436-Vascular Anatomy - VilelaashleyNo ratings yet
- Midbrain, Pons, and Medulla: Anatomy and SyndromesDocument16 pagesMidbrain, Pons, and Medulla: Anatomy and SyndromesJasper CubiasNo ratings yet
- COSDocument82 pagesCOSSPRTOSHBTINo ratings yet
- 3D Sequence For Lumbar Nerve Root With Interverbetbral Foramen COSMICDocument6 pages3D Sequence For Lumbar Nerve Root With Interverbetbral Foramen COSMICkhamsenglNo ratings yet
- (19330715 - Journal of Neurosurgery - Pediatrics) Selective Dorsal Rhizotomy - An Illustrated Review of Operative TechniquesDocument8 pages(19330715 - Journal of Neurosurgery - Pediatrics) Selective Dorsal Rhizotomy - An Illustrated Review of Operative Techniquesclinica vet ensenadaNo ratings yet
- Utility of Mri in The Early and Accurate Diagnosis of Avascular Necrosis of Hip JointDocument9 pagesUtility of Mri in The Early and Accurate Diagnosis of Avascular Necrosis of Hip JointDenis AlexandruNo ratings yet
- Juxtacortical Lesions and Cortical Thinning in Multiple SclerosisDocument7 pagesJuxtacortical Lesions and Cortical Thinning in Multiple SclerosishelenNo ratings yet
- Fernandez-Miranda JC. 2007 - Three-Dimensional Microsurgical and Tractographic Anatomy of The White Matter..Document40 pagesFernandez-Miranda JC. 2007 - Three-Dimensional Microsurgical and Tractographic Anatomy of The White Matter..Beyza ZeyrekNo ratings yet
- The Clinical Correlation of A New Practical MRI Method For Grading Cervical Neural Foraminal Stenosis Based On Oblique Sagittal ImagesDocument6 pagesThe Clinical Correlation of A New Practical MRI Method For Grading Cervical Neural Foraminal Stenosis Based On Oblique Sagittal ImagesThiago Astil RizzettoNo ratings yet
- Bahan 3Document11 pagesBahan 3Adam JohnsonNo ratings yet
- Synchronous Spike DischargeDocument20 pagesSynchronous Spike DischargeAmey MoreNo ratings yet
- Muscle & Nerve Volume 15 Issue 3 1992 (Doi 10 - CopiarDocument10 pagesMuscle & Nerve Volume 15 Issue 3 1992 (Doi 10 - CopiarPile BallNo ratings yet
- Anatomy of Cauda EquinaDocument4 pagesAnatomy of Cauda EquinaacscribNo ratings yet
- 1 s2.0 S1053811923003348 MainDocument15 pages1 s2.0 S1053811923003348 MainPeggy WangNo ratings yet
- Magnetic Resonance Imaging - 2013 - Ignjatovi - Brain Iron MRI A Biomarker For Amyotrophic Lateral SclerosisDocument8 pagesMagnetic Resonance Imaging - 2013 - Ignjatovi - Brain Iron MRI A Biomarker For Amyotrophic Lateral SclerosisMahima vermaNo ratings yet
- Diagnostic Implication and Clinical Relevance of Dermatomal Somatosensory Evoked Potentials in Patients With RadiculopathyDocument7 pagesDiagnostic Implication and Clinical Relevance of Dermatomal Somatosensory Evoked Potentials in Patients With RadiculopathyLuciano RuizNo ratings yet
- MRI Neonatal Brain PDFDocument12 pagesMRI Neonatal Brain PDFWorthless BoysNo ratings yet
- Pictorial Essay of Cranial Nerves Lesions On MRI Our ExperienceDocument10 pagesPictorial Essay of Cranial Nerves Lesions On MRI Our ExperienceAamir YousufNo ratings yet
- Skeletal Development of The Proximal Humerus in The Pediatric Population: MRI FeaturesDocument10 pagesSkeletal Development of The Proximal Humerus in The Pediatric Population: MRI Featuresahmed doweidarNo ratings yet
- Neuroplasticity Changes with Exercise in Older AdultsDocument28 pagesNeuroplasticity Changes with Exercise in Older AdultsMahi KatreNo ratings yet
- MRI Sequences Comparison for Microbleeds DetectionDocument7 pagesMRI Sequences Comparison for Microbleeds DetectionMuhammad SawalNo ratings yet
- Descriptive Study of The Differences in The Level of The Conus Medullaris in Four Different Age GroupsDocument7 pagesDescriptive Study of The Differences in The Level of The Conus Medullaris in Four Different Age GroupsregarskidNo ratings yet
- MRI of Spinal Cord P1Document6 pagesMRI of Spinal Cord P1BenjaminNo ratings yet
- Automatic Tissue Segmentation With Deep Learning in Patients With Congenital or Acquired Distortion of Brain Anatomy (Preprint)Document12 pagesAutomatic Tissue Segmentation With Deep Learning in Patients With Congenital or Acquired Distortion of Brain Anatomy (Preprint)Denis PeruzzoNo ratings yet
- Sensory Neural Conduction of Median Nerv PDFDocument5 pagesSensory Neural Conduction of Median Nerv PDFemilio9fernandez9gatNo ratings yet
- Fpsyt 11 00440Document12 pagesFpsyt 11 00440humanknowledge4No ratings yet
- Neuroimage: Justin Ales, Thom Carney, Stanley A. KleinDocument9 pagesNeuroimage: Justin Ales, Thom Carney, Stanley A. KleinnikadonNo ratings yet
- Imaging The Spine: Orthopaedics E Ii: Spine and PelvisDocument13 pagesImaging The Spine: Orthopaedics E Ii: Spine and Pelvisraul ramboyongNo ratings yet
- Berning 2012Document1 pageBerning 2012László SágiNo ratings yet
- Yue Et Al 2023 Validity Study of A Multiscaled Fusion Network Using Single Lead Electrocardiogram Signals ForDocument9 pagesYue Et Al 2023 Validity Study of A Multiscaled Fusion Network Using Single Lead Electrocardiogram Signals Forrezaferidooni00No ratings yet
- Uas CT Scan - Jurnal - Dwi Ajeng Risqy Hasanah Syam - P1337430219162 PDFDocument6 pagesUas CT Scan - Jurnal - Dwi Ajeng Risqy Hasanah Syam - P1337430219162 PDFDwi Ajeng Risqy HasanahSyamNo ratings yet
- Regional Homogeneity Analysis On Acupoint.19Document6 pagesRegional Homogeneity Analysis On Acupoint.19JouleAlSBNo ratings yet
- Quantitative Characterization of Optic Nerve Atrophy in Patients With Multiple SclerosisDocument8 pagesQuantitative Characterization of Optic Nerve Atrophy in Patients With Multiple SclerosisSulmiawati SyamNo ratings yet
- Jurnal IlmiahDocument8 pagesJurnal IlmiahDeni Ratna Juwita IINo ratings yet
- 2019-TMI-Cardiac Phase Detection in EchocardiogramsDocument12 pages2019-TMI-Cardiac Phase Detection in EchocardiogramsZhenyu BuNo ratings yet
- Analysis of Clinical and Electrophysiological CharacteristicsDocument7 pagesAnalysis of Clinical and Electrophysiological CharacteristicsAurelia Sartika TongkuNo ratings yet
- AsDocument21 pagesAsOtong Zam Zamy75% (4)
- Ajr 08 2286Document9 pagesAjr 08 2286Otong Zam ZamyNo ratings yet
- AsdDocument15 pagesAsdOtong Zam ZamyNo ratings yet
- CFAC Guide - Ankle LigamentsDocument12 pagesCFAC Guide - Ankle LigamentsOtong Zam ZamyNo ratings yet
- Slimmon Brukner AFP 2010 AnkleDocument5 pagesSlimmon Brukner AFP 2010 AnkleOtong Zam ZamyNo ratings yet
- JBiSE 2013032916535602Document8 pagesJBiSE 2013032916535602Otong Zam ZamyNo ratings yet
- Exercise 4Document9 pagesExercise 4Toni Chifligaroski100% (1)
- Mri of Sports-Related Injuries of The Foot and Ankle - Part 1Document17 pagesMri of Sports-Related Injuries of The Foot and Ankle - Part 1Otong Zam ZamyNo ratings yet
- Comparison of Fast Spin-Echo Versus Conventional Spin-Echo MRI For Evaluating Meniscal TearsDocument4 pagesComparison of Fast Spin-Echo Versus Conventional Spin-Echo MRI For Evaluating Meniscal TearsOtong Zam ZamyNo ratings yet
- MR Imaging of Disorders of The Achilles TendonDocument14 pagesMR Imaging of Disorders of The Achilles TendonOtong Zam ZamyNo ratings yet
- Anterior Talofbular Ligament RuptureRepair and Reinforcement Using DermaSpan Acellular Dermal MatrixDocument2 pagesAnterior Talofbular Ligament RuptureRepair and Reinforcement Using DermaSpan Acellular Dermal MatrixOtong Zam ZamyNo ratings yet
- Improvements in Lumbar Spine MRI at 3 T Using Parallel TransmissionDocument7 pagesImprovements in Lumbar Spine MRI at 3 T Using Parallel TransmissionOtong Zam ZamyNo ratings yet
- Anterior Talofbular Ligament RuptureRepair and Reinforcement Using DermaSpan Acellular Dermal MatrixDocument2 pagesAnterior Talofbular Ligament RuptureRepair and Reinforcement Using DermaSpan Acellular Dermal MatrixOtong Zam ZamyNo ratings yet
- MR Imaging of Disorders of The Achilles TendonDocument14 pagesMR Imaging of Disorders of The Achilles TendonOtong Zam ZamyNo ratings yet
- 03668Document1 page03668Otong Zam ZamyNo ratings yet
- Contrast Reactions HSGDocument67 pagesContrast Reactions HSGOtong Zam ZamyNo ratings yet
- Herniation of Cartilaginous Endplates in The Lumbar Spine MRI FindingsDocument7 pagesHerniation of Cartilaginous Endplates in The Lumbar Spine MRI FindingsOtong Zam ZamyNo ratings yet
- Axial Compression Frame For MRI of Thoracolumbar SpineDocument4 pagesAxial Compression Frame For MRI of Thoracolumbar SpineOtong Zam ZamyNo ratings yet
- MRI of The Spine and Spinal Cord: Imaging Techniques, Normal Anatomy, Artifacts, and PitfallsDocument6 pagesMRI of The Spine and Spinal Cord: Imaging Techniques, Normal Anatomy, Artifacts, and PitfallsOtong Zam ZamyNo ratings yet
- Accuracy of 3-T MRI Using Fast Spin-Echo Technique To Detect Meniscal Tears of The KneeDocument5 pagesAccuracy of 3-T MRI Using Fast Spin-Echo Technique To Detect Meniscal Tears of The KneeOtong Zam ZamyNo ratings yet
- Contrast Reactions HSGDocument67 pagesContrast Reactions HSGOtong Zam ZamyNo ratings yet
- Vertebral Column: Osteology and ArthrologyDocument75 pagesVertebral Column: Osteology and ArthrologyGeorge WangNo ratings yet
- Introduction To Musculosceletal CTDocument50 pagesIntroduction To Musculosceletal CTOtong Zam ZamyNo ratings yet
- Contrast Reactions HSGDocument67 pagesContrast Reactions HSGOtong Zam ZamyNo ratings yet
- Contrast Reactions HSGDocument67 pagesContrast Reactions HSGOtong Zam ZamyNo ratings yet
- Contrast NephropathyDocument21 pagesContrast NephropathyOtong Zam ZamyNo ratings yet
- MRI Physics 2: Contrasts and Protocols: Chris Rorden Types of Contrast: ProtocolsDocument31 pagesMRI Physics 2: Contrasts and Protocols: Chris Rorden Types of Contrast: ProtocolsOtong Zam ZamyNo ratings yet
- Vertebral ColumnDocument26 pagesVertebral ColumnOtong Zam ZamyNo ratings yet
- PembatasDocument1 pagePembatasOtong Zam ZamyNo ratings yet
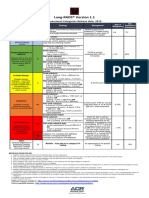
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 pageLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNo ratings yet
- HEPATITIS B VACCINE NURSING RESPONSIBILITIESDocument14 pagesHEPATITIS B VACCINE NURSING RESPONSIBILITIESJannine BensiNo ratings yet
- COVID-19 Patient Report SummaryDocument2 pagesCOVID-19 Patient Report Summarymuhammad imranNo ratings yet
- Journal BalakrishnaDocument3 pagesJournal BalakrishnafandheanayaNo ratings yet
- 6 5 Nerves Hormones and HomeostasisDocument19 pages6 5 Nerves Hormones and Homeostasisapi-235355872No ratings yet
- Case Study PneumothoraxDocument9 pagesCase Study PneumothoraxLee_Cabral_693967% (3)
- Oral Health During Pregnancy - An Analysis of Information CoDocument8 pagesOral Health During Pregnancy - An Analysis of Information CoElena IancuNo ratings yet
- KenyaEMR v17.3.1 Release Notes SummaryDocument3 pagesKenyaEMR v17.3.1 Release Notes SummaryMigori Art DataNo ratings yet
- Optima GutDocument11 pagesOptima GutNoly ClaveringNo ratings yet
- National Institute of Occupational Safety and Health Course CurriculumDocument9 pagesNational Institute of Occupational Safety and Health Course Curriculummohan dassNo ratings yet
- Position Paper On Teenage PregnancyDocument3 pagesPosition Paper On Teenage PregnancyMark Anthony CabangonNo ratings yet
- The Natural Way To A Healthy HealingDocument111 pagesThe Natural Way To A Healthy HealingAnjanaNo ratings yet
- Psoriasis and Miracles With HomoeopathyDocument3 pagesPsoriasis and Miracles With HomoeopathyEditor IJTSRDNo ratings yet
- Medical Assessment Form Blank-1Document4 pagesMedical Assessment Form Blank-1Zakiya HassanNo ratings yet
- Dental CatalogueDocument28 pagesDental CataloguePaulus LagadanNo ratings yet
- ImmunosuppresentsDocument13 pagesImmunosuppresentsmadeputraNo ratings yet
- Assignment 1 Cs 0902Document4 pagesAssignment 1 Cs 0902prince12No ratings yet
- DUODENAL PROCEDUREDocument5 pagesDUODENAL PROCEDUREeka nurjanahNo ratings yet
- Kasus Farter 2 10 Mei 2019Document3 pagesKasus Farter 2 10 Mei 2019YonicaryanNo ratings yet
- 2012 Karshaniya YavaguDocument4 pages2012 Karshaniya YavaguRANJEET SAWANTNo ratings yet
- Ann JeinaDocument7 pagesAnn JeinaMizumoriFumairaNo ratings yet
- Definition of NephrolithiasisDocument30 pagesDefinition of Nephrolithiasiszz_13No ratings yet
- Unipex Onepager CapixylDocument1 pageUnipex Onepager CapixylalbertitorubinNo ratings yet
- Hipertensi Portal Donny SandraDocument67 pagesHipertensi Portal Donny SandrabobyNo ratings yet