You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- DfsdfsDocument12 pagesDfsdfsSitiKhadijahNo ratings yet
- Christensen 2008Document4 pagesChristensen 2008SitiKhadijahNo ratings yet
- 2004 EndodtopicsHaapasaloetal PDFDocument28 pages2004 EndodtopicsHaapasaloetal PDFSitiKhadijahNo ratings yet
- X-Smart Plus Brochure Maillefer Badge enDocument3 pagesX-Smart Plus Brochure Maillefer Badge enSitiKhadijahNo ratings yet
- Boss Hard 2017Document10 pagesBoss Hard 2017SitiKhadijahNo ratings yet
- Hoferl 2015Document6 pagesHoferl 2015SitiKhadijahNo ratings yet
- 2004 EndodtopicsHaapasaloetalDocument8 pages2004 EndodtopicsHaapasaloetalSitiKhadijahNo ratings yet
- Postgraduate Department of Conservative Dentistry and EndodonticsDocument125 pagesPostgraduate Department of Conservative Dentistry and EndodonticsSitiKhadijahNo ratings yet
- Review Article: A New Classification of Endodontic-Periodontal LesionsDocument6 pagesReview Article: A New Classification of Endodontic-Periodontal LesionsSitiKhadijahNo ratings yet
- 90Document5 pages90SitiKhadijahNo ratings yet
- Fracture Reaons in PFMDocument5 pagesFracture Reaons in PFMShounak GhoshNo ratings yet
- Identification of Complete Denture Problems: A Summary: ProstheticsDocument7 pagesIdentification of Complete Denture Problems: A Summary: ProstheticsPolo RalfNo ratings yet
- Sol Ruz 2015Document7 pagesSol Ruz 2015SitiKhadijahNo ratings yet
- 1548 FullDocument9 pages1548 FullSitiKhadijahNo ratings yet
- Managment of Wear2Document7 pagesManagment of Wear2hmsatNo ratings yet
- Implant-Retained Cantilever Fixed Prosthesis: Where and WhenDocument4 pagesImplant-Retained Cantilever Fixed Prosthesis: Where and WhenSitiKhadijahNo ratings yet
- CantileverDocument6 pagesCantileverSitiKhadijahNo ratings yet
- f26f PDFDocument9 pagesf26f PDFSitiKhadijahNo ratings yet
- Effect of EDTA Sodium Hypochlorite and C PDFDocument4 pagesEffect of EDTA Sodium Hypochlorite and C PDFZulfahmi NurdinNo ratings yet
- Gurrea Bruguera IJED 2014Document18 pagesGurrea Bruguera IJED 2014SitiKhadijahNo ratings yet
- 2014 02 05 LimTongWahDocument6 pages2014 02 05 LimTongWahSitiKhadijahNo ratings yet
- Removable Prostheses: Tooth Surface LossDocument4 pagesRemovable Prostheses: Tooth Surface LossSitiKhadijahNo ratings yet
- BDA Occlusion Seminar 2Document88 pagesBDA Occlusion Seminar 2SitiKhadijahNo ratings yet
- TJ Der Hane 2009Document33 pagesTJ Der Hane 2009SitiKhadijahNo ratings yet
- Applied-A Comparative Evaluation-Shweta BagmarDocument8 pagesApplied-A Comparative Evaluation-Shweta BagmarImpact JournalsNo ratings yet
- Mixed Designs: Between and Within: Psy 420 AinsworthDocument30 pagesMixed Designs: Between and Within: Psy 420 AinsworthSitiKhadijahNo ratings yet
- Ataali 2014Document9 pagesAtaali 2014SitiKhadijahNo ratings yet
- 10 1046@j 1365-2591 2000 00273 XDocument7 pages10 1046@j 1365-2591 2000 00273 XSitiKhadijahNo ratings yet
- 11 SPSS Procedure For Kruskal Wallis TestDocument5 pages11 SPSS Procedure For Kruskal Wallis TestSitiKhadijahNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hot Aishwarya Rai Wedding and Her Life.20130105.040216Document2 pagesThe Hot Aishwarya Rai Wedding and Her Life.20130105.040216anon_501746111100% (1)
- Open Book Online: Syllabus & Pattern Class - XiDocument1 pageOpen Book Online: Syllabus & Pattern Class - XiaadityaNo ratings yet
- Training Structure - Thinkific Plus TemplateDocument7 pagesTraining Structure - Thinkific Plus TemplateQIONG WUNo ratings yet
- Oxygenation - NCPDocument5 pagesOxygenation - NCPCazze SunioNo ratings yet
- Prelims CB em Ii5Document21 pagesPrelims CB em Ii5Ugaas SareeyeNo ratings yet
- Attitude of Tribal and Non Tribal Students Towards ModernizationDocument9 pagesAttitude of Tribal and Non Tribal Students Towards ModernizationAnonymous CwJeBCAXpNo ratings yet
- New Horizon Public School, Airoli: Grade X: English: Poem: The Ball Poem (FF)Document42 pagesNew Horizon Public School, Airoli: Grade X: English: Poem: The Ball Poem (FF)stan.isgod99No ratings yet
- Vermicomposting Learning ModulesDocument6 pagesVermicomposting Learning ModulesPamara Prema Khannae100% (1)
- Outbound Idocs Code Error Event Severity Sap MeaningDocument2 pagesOutbound Idocs Code Error Event Severity Sap MeaningSummit YerawarNo ratings yet
- The Impact of Online Games To The AcademicDocument20 pagesThe Impact of Online Games To The AcademicJessica BacaniNo ratings yet
- Leonard Nadler' ModelDocument3 pagesLeonard Nadler' ModelPiet Gabz67% (3)
- COE301 Lab 2 Introduction MIPS AssemblyDocument7 pagesCOE301 Lab 2 Introduction MIPS AssemblyItz Sami UddinNo ratings yet
- Practical Research 2 Group 11 RRL, Proposed Title and Answers To The QuestionsDocument14 pagesPractical Research 2 Group 11 RRL, Proposed Title and Answers To The QuestionsFeby Margaret AngNo ratings yet
- Important Instructions For Winter-2020 MCQ Based Online ExaminationDocument1 pageImportant Instructions For Winter-2020 MCQ Based Online Examinationdenoh32751No ratings yet
- Sailpoint Topic Wise SyllabusDocument2 pagesSailpoint Topic Wise SyllabusKishore KodaliNo ratings yet
- Limited Alembic: Employee Related DataDocument4 pagesLimited Alembic: Employee Related DataTp EarningsNo ratings yet
- MGN815: Business Models: Ajay ChandelDocument38 pagesMGN815: Business Models: Ajay ChandelSam RehmanNo ratings yet
- Epson EcoTank ITS Printer L4150 DatasheetDocument2 pagesEpson EcoTank ITS Printer L4150 DatasheetWebAntics.com Online Shopping StoreNo ratings yet
- Hssive-Xi-Chem-4. Chemical Bonding and Molecular Structure Q & ADocument11 pagesHssive-Xi-Chem-4. Chemical Bonding and Molecular Structure Q & AArties MNo ratings yet
- RA-035659 - CIVIL ENGINEER - Cebu - 5-2022Document157 pagesRA-035659 - CIVIL ENGINEER - Cebu - 5-2022Ash AlbainNo ratings yet
- The Politics of GenreDocument21 pagesThe Politics of GenreArunabha ChaudhuriNo ratings yet
- ZEROPAY WhitepaperDocument15 pagesZEROPAY WhitepaperIlham NurrohimNo ratings yet
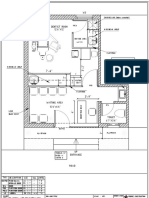
- Dental Clinic - Floor Plan R3-2Document1 pageDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- TVL-SMAW 12 - Week 4 - Lesson 1 - Concept of Welding Codes and StandardsDocument9 pagesTVL-SMAW 12 - Week 4 - Lesson 1 - Concept of Welding Codes and StandardsNelPalalonNo ratings yet
- Statistics and Probability Course Syllabus (2023) - SignedDocument3 pagesStatistics and Probability Course Syllabus (2023) - SignedDarence Fujihoshi De AngelNo ratings yet
- LG) Pc-Ii Formulation of Waste Management PlansDocument25 pagesLG) Pc-Ii Formulation of Waste Management PlansAhmed ButtNo ratings yet
- Dokumen - Tips - Dominick Salvatore Microeconomics Wwwpdfsdocuments2comd38dominick SalvatorepdfDocument2 pagesDokumen - Tips - Dominick Salvatore Microeconomics Wwwpdfsdocuments2comd38dominick SalvatorepdfIshan SharmaNo ratings yet
- Norm ANSI PDFDocument1 pageNorm ANSI PDFAbdul Quddus Mat IsaNo ratings yet
- American University of Beirut PSPA 210: Intro. To Political ThoughtDocument4 pagesAmerican University of Beirut PSPA 210: Intro. To Political Thoughtcharles murrNo ratings yet
- Amazon VS WalmartDocument5 pagesAmazon VS WalmartBrandy M. Twilley100% (1)