You might also like
- QMS 140 Root Cause Analysis Investigation Procedure SampleDocument3 pagesQMS 140 Root Cause Analysis Investigation Procedure Samplex engineeringNo ratings yet
- Root Cause AnalysisDocument9 pagesRoot Cause AnalysisAl Engg100% (9)
- Implementing An Effective Capa Process: Sue Jacobs Cecilia Kimberlin, PHDDocument33 pagesImplementing An Effective Capa Process: Sue Jacobs Cecilia Kimberlin, PHDPratyNo ratings yet
- Root Cause AnalysisDocument16 pagesRoot Cause AnalysisBryan NguyenNo ratings yet
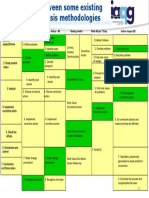
- Root Cause Analysis Methodologies IAQGDocument1 pageRoot Cause Analysis Methodologies IAQGAldo100% (1)
- Fmea Process TemplateDocument20 pagesFmea Process TemplateLazarasBenny IsprithiyoneNo ratings yet
- Root Cause AnalysisDocument56 pagesRoot Cause AnalysisDhana Raju100% (1)
- Root Cause Analysis (RCA)Document20 pagesRoot Cause Analysis (RCA)Shieradel Jimenez100% (1)
- Root Cause Analysis ReportDocument3 pagesRoot Cause Analysis Reportnesmanila3219No ratings yet
- 5 Why Root Cause AnalysisDocument1 page5 Why Root Cause AnalysisSinan İcik100% (1)
- Root Cause Analysis Course OverviewDocument102 pagesRoot Cause Analysis Course Overviewwaran87100% (1)
- Arc Flash Study The Six Steps PDFDocument7 pagesArc Flash Study The Six Steps PDFCarlos Lino Rojas AgüeroNo ratings yet
- Root Cause Analysis ToolDocument1 pageRoot Cause Analysis ToolZakiSaa0% (1)
- 5 Why AnalysisDocument55 pages5 Why AnalysisHarshit Sharma100% (1)
- Root Cause AnalysisDocument16 pagesRoot Cause AnalysisPat TejNo ratings yet
- 5 WHYs ROOT CAUSE ANALYSIS TEMPLATEDocument2 pages5 WHYs ROOT CAUSE ANALYSIS TEMPLATEAjiwuriNo ratings yet
- Checklist: Mobile Crane SafetyDocument2 pagesChecklist: Mobile Crane SafetyJohn Kurong100% (5)
- Root Causes AnalisysDocument33 pagesRoot Causes Analisysandrés_donossoNo ratings yet
- Root Cause Analysis PresentationDocument37 pagesRoot Cause Analysis PresentationucheonixNo ratings yet
- 5 Whys TrainingDocument14 pages5 Whys TrainingPanch BNo ratings yet
- Cause and Effect Diagram: CA/PA-RCA: Basic ToolDocument21 pagesCause and Effect Diagram: CA/PA-RCA: Basic Toolsiddiquiee74100% (1)
- RCA Framework Root Cause AnalysisDocument11 pagesRCA Framework Root Cause Analysisbenaoumeur benouna100% (1)
- Root Cause Analysis: Coronet Foods Pvt. LTDDocument103 pagesRoot Cause Analysis: Coronet Foods Pvt. LTDSaif Sultan0% (1)
- Why Why Analysis - Making Smart Decisions Based On Root CauseDocument5 pagesWhy Why Analysis - Making Smart Decisions Based On Root CauseThilagavathy Palaniappan100% (1)
- Root Cause AnalysisDocument28 pagesRoot Cause Analysisaftabseven2No ratings yet
- Root Cause Analysis - ToolDocument11 pagesRoot Cause Analysis - ToolFouzan SoniwalaNo ratings yet
- Root Cause Analysis 27.3.19Document43 pagesRoot Cause Analysis 27.3.19Musical CorruptionNo ratings yet
- S6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Document26 pagesS6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Rona Dindang100% (1)
- Eight Disciplines of Problem Solving (8D) ExplainedDocument7 pagesEight Disciplines of Problem Solving (8D) Explained@yuanNo ratings yet
- FMEA - A Guide For Continuous ImprovementDocument36 pagesFMEA - A Guide For Continuous Improvementvipin_chaudhary100% (1)
- 6 Methods of Verifying CAPADocument3 pages6 Methods of Verifying CAPAMariver LlorenteNo ratings yet
- 6.water Treatment and Make-Up Water SystemDocument18 pages6.water Treatment and Make-Up Water Systempepenapao1217100% (1)
- Chapter 06 Solutions PDFDocument15 pagesChapter 06 Solutions PDFkareem3456No ratings yet
- Root Cause Analysis MPM1-GlDocument39 pagesRoot Cause Analysis MPM1-GlJunaid KhanNo ratings yet
- 8d-Report (Ishikawa)Document12 pages8d-Report (Ishikawa)Miro Vincek100% (1)
- Training On Root Cause Analysis / Problem Solving TechniquesDocument66 pagesTraining On Root Cause Analysis / Problem Solving TechniquesDINESH SHARMANo ratings yet
- 8D Report Training MIDDocument23 pages8D Report Training MIDanon_86320488No ratings yet
- Why, Why Root Cause AnalysisDocument1 pageWhy, Why Root Cause AnalysisRodarbal Zerimar HtebNo ratings yet
- Eight Disciplines of Problem SolvingDocument4 pagesEight Disciplines of Problem Solvingshiivendra100% (1)
- 5 Whys Root Cause Analysis Worksheet SampleDocument4 pages5 Whys Root Cause Analysis Worksheet SampleSANJOY MAJINo ratings yet
- Root Cause AnalysisDocument5 pagesRoot Cause Analysistamara_002150% (2)
- Final Session Guide Root CauseDocument11 pagesFinal Session Guide Root CauseBagamel YlananNo ratings yet
- Loop Checking and Field Instrument Testing ProcedureDocument7 pagesLoop Checking and Field Instrument Testing Procedurecharzree0% (1)
- Problem Solution - 5 Whys Analysis WorksheetDocument3 pagesProblem Solution - 5 Whys Analysis WorksheetbhushansalunkeNo ratings yet
- Installation Settings IssueDocument4 pagesInstallation Settings IssueG. Vijaykumar Rao100% (1)
- 5 WhysDocument2 pages5 WhysJim Adams100% (1)
- 5 S Principles ExplainedDocument30 pages5 S Principles Explainedamaresh nkNo ratings yet
- Heal Yourself in Ten Minutes AJDocument9 pagesHeal Yourself in Ten Minutes AJJason Mangrum100% (1)
- SIPOC: A Six Sigma Tool Helping On ISO 9000 Quality Management SystemsDocument10 pagesSIPOC: A Six Sigma Tool Helping On ISO 9000 Quality Management SystemsYogesh ChavanNo ratings yet
- Inspection and Test Plan: Flow Chart Start IncomingDocument1 pageInspection and Test Plan: Flow Chart Start IncomingSinden AyuNo ratings yet
- NOC Processes GuideDocument26 pagesNOC Processes GuideCamille Bertrand Kite100% (1)
- Root Cause AnalysisDocument5 pagesRoot Cause AnalysisNishabharatNo ratings yet
- Root Cause Analysis ToolsDocument15 pagesRoot Cause Analysis ToolscmlimNo ratings yet
- Cause and Effect DiagramsDocument4 pagesCause and Effect DiagramsMohammad Jaid AlamNo ratings yet
- Applied Root Cause Analysis, Part 2Document4 pagesApplied Root Cause Analysis, Part 2caddleman100% (1)
- Instructions: © 2010 Know Ware International IncDocument3 pagesInstructions: © 2010 Know Ware International Incpinkcity2013No ratings yet
- 5 Why Root Cause AnalysisDocument3 pages5 Why Root Cause AnalysisDaniswara Krisna PrabathaNo ratings yet
- Falls - Root Cause Analysis FinalDocument1 pageFalls - Root Cause Analysis FinalMohammed KhatibNo ratings yet
- Cause Mapping Template: Explain The ProblemDocument7 pagesCause Mapping Template: Explain The Problem25aprilNo ratings yet
- Fishbone Analysis StudyGuideDocument7 pagesFishbone Analysis StudyGuideJulrick Cubio Egbus100% (1)
- Root Cause Analysis TemplateDocument2 pagesRoot Cause Analysis TemplateJames Wigglesworth SantilliNo ratings yet
- Guided By: Prof. A. D. PatilDocument14 pagesGuided By: Prof. A. D. Patilshubham puranikNo ratings yet
- Quality Assurance Vs ControlDocument3 pagesQuality Assurance Vs ControlYay B. GicoNo ratings yet
- 3 Root Cause Analysis TemplateDocument4 pages3 Root Cause Analysis TemplatenensyNo ratings yet
- Project Monitoring and ControllingDocument7 pagesProject Monitoring and ControllingTadele DandenaNo ratings yet
- Failure Analysis ProcessDocument3 pagesFailure Analysis ProcessAnonymous LaV8mFnemNo ratings yet
- Process Piping in Spec ProgramsDocument8 pagesProcess Piping in Spec Programsdineshkumark1986No ratings yet
- Progm - 9-8-18 FinalDocument2 pagesProgm - 9-8-18 Finalkareem3456No ratings yet
- Supply Chain Management Spring 2018 Case Course OutlineDocument6 pagesSupply Chain Management Spring 2018 Case Course Outlinekareem3456No ratings yet
- Ground Floor Hall, Offices, Ticket Booths, Information Center, Waiting AreaDocument1 pageGround Floor Hall, Offices, Ticket Booths, Information Center, Waiting Areakareem3456No ratings yet
- TVM NetDocument24 pagesTVM Netkareem3456No ratings yet
- Chapter 06 Adobe - 2Document1 pageChapter 06 Adobe - 2kareem3456No ratings yet
- Basharat 32 18 230 Nasir 179 4 23 Imran Riaz 25 11 142 Adnan Riaz 80 105 11 142Document1 pageBasharat 32 18 230 Nasir 179 4 23 Imran Riaz 25 11 142 Adnan Riaz 80 105 11 142kareem3456No ratings yet
- Solved Questions - PaperDocument1 pageSolved Questions - Paperkareem3456No ratings yet
- Date Subject Task Tasked byDocument2 pagesDate Subject Task Tasked bykareem3456No ratings yet
- Tender Inquiry For Stall Construction Ukrai-2017 On (23!8!2017)Document13 pagesTender Inquiry For Stall Construction Ukrai-2017 On (23!8!2017)kareem3456No ratings yet
- IonDocument1 pageIonkareem3456No ratings yet
- Network DiagramsDocument8 pagesNetwork Diagramscrystal50% (2)
- SOP for coordinating with defence attaché officesDocument1 pageSOP for coordinating with defence attaché officeskareem3456No ratings yet
- Em'S Obligations Ser Obligations RemarksDocument3 pagesEm'S Obligations Ser Obligations Remarkskareem3456No ratings yet
- 'Goat FarmDocument1 page'Goat Farmkareem3456No ratings yet
- 6Document1 page6kareem3456No ratings yet
- World ExhibitionsDocument1 pageWorld Exhibitionskareem3456No ratings yet
- HowtodoitDocument1 pageHowtodoitkareem3456No ratings yet
- 1Document1 page1kareem3456No ratings yet
- 6Document1 page6kareem3456No ratings yet
- 6Document1 page6kareem3456No ratings yet
- 1Document1 page1kareem3456No ratings yet
- 5Document1 page5kareem3456No ratings yet
- 8Document1 page8kareem3456No ratings yet
- 6Document1 page6kareem3456No ratings yet
- 5Document1 page5kareem3456No ratings yet
- 5Document1 page5kareem3456No ratings yet
- Compulsory Papers - EmailDocument2 pagesCompulsory Papers - Emailkareem3456No ratings yet
- Launch Strategies 1. Penetration Strategy Is Based On Low Prices, Being Recommended When Company Aims To Encourage Demand (To Attract Customers) and Expand Its Market, While Growing Profits BasedDocument1 pageLaunch Strategies 1. Penetration Strategy Is Based On Low Prices, Being Recommended When Company Aims To Encourage Demand (To Attract Customers) and Expand Its Market, While Growing Profits Basedkareem3456No ratings yet
- HR 1Document1 pageHR 1kareem3456No ratings yet
- Volume 1Document168 pagesVolume 1lalitendu jenaNo ratings yet
- Climate Change and Global Warming and Its Impact On BangladeshDocument7 pagesClimate Change and Global Warming and Its Impact On BangladeshAminulHoqueNo ratings yet
- Causes of Failure of Earth DamsDocument11 pagesCauses of Failure of Earth DamsThéoneste NSANZIMFURANo ratings yet
- TSB 20230831 - Reconnect FATL WM Error Code & Troubleshooting GuideDocument6 pagesTSB 20230831 - Reconnect FATL WM Error Code & Troubleshooting GuideNavjot KaurNo ratings yet
- H1 Revision Notes DNA and GenomicsDocument6 pagesH1 Revision Notes DNA and GenomicsJiaLi XieNo ratings yet
- Ielts Band Score 7Document2 pagesIelts Band Score 7Subhan Iain IINo ratings yet
- Vietnam Snack Market Grade BDocument3 pagesVietnam Snack Market Grade BHuỳnh Điệp TrầnNo ratings yet
- Cswip Visual Welding Inspector 3.0 BrochureDocument1 pageCswip Visual Welding Inspector 3.0 BrochureNasfauzan100% (2)
- EFPSDocument8 pagesEFPSBryan Joshua VillarNo ratings yet
- 2VV-33C-R4-V5 Product SpecificationsDocument5 pages2VV-33C-R4-V5 Product Specificationsnhan sieuNo ratings yet
- Somali Guideline of InvestorsDocument9 pagesSomali Guideline of InvestorsABDULLAHI HAGAR FARAH HERSI STUDENTNo ratings yet
- G. Metals and NonmetalsDocument26 pagesG. Metals and NonmetalsKyzer Calix LaguitNo ratings yet
- Rundingan Perdagangan Antara Malaysia Dan Indonesia Di Wisma Putra, Kuala Lumpur 1967Document15 pagesRundingan Perdagangan Antara Malaysia Dan Indonesia Di Wisma Putra, Kuala Lumpur 1967nixyingboNo ratings yet
- Regulation of Body FluidsDocument7 pagesRegulation of Body FluidsRuth FamillaranNo ratings yet
- Radiol 2020201473Document37 pagesRadiol 2020201473M Victoria SalazarNo ratings yet
- Corn Pulao Recipe With Sweet CornDocument2 pagesCorn Pulao Recipe With Sweet CornSudharshanNo ratings yet
- Honda PCX150Document137 pagesHonda PCX150Akchu KadNo ratings yet
- PTA Resolution for Donation to School WashroomDocument2 pagesPTA Resolution for Donation to School WashroomMara Ciela CajalneNo ratings yet
- WHO COVID-19 Situation Report - July 11Document16 pagesWHO COVID-19 Situation Report - July 11CityNewsTorontoNo ratings yet
- Balloons FullDocument19 pagesBalloons FullHoan Doan NgocNo ratings yet
- 4Document130 pages4Upender BhatiNo ratings yet
- Ethnobotany Manual 14th September 2016Document54 pagesEthnobotany Manual 14th September 2016Rahul0% (1)
- Jamec Air FittingsDocument18 pagesJamec Air Fittingsgoeez1No ratings yet
- SSMT ConplanDocument2 pagesSSMT ConplanJeffrey VillangcaNo ratings yet