You might also like
- Mohd Azzarain Bin Abdul Aziz: Injection WithdrawalDocument2 pagesMohd Azzarain Bin Abdul Aziz: Injection WithdrawalAffeif AzzarainNo ratings yet
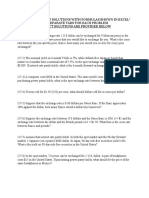
- Chapter 17 Homework ProblemsDocument5 pagesChapter 17 Homework ProblemsAarti JNo ratings yet
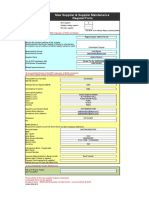
- Vendor Registration FormDocument3 pagesVendor Registration FormDanish Naeem LambeNo ratings yet
- KYC Modification Format - Jan 2021Document1 pageKYC Modification Format - Jan 2021Vishwanath SagawkarNo ratings yet
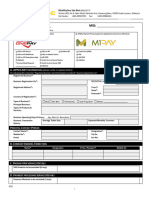
- MERCHANT REQUEST FORM - Paydee SDN BHDDocument2 pagesMERCHANT REQUEST FORM - Paydee SDN BHDKeerthiga ManoharanNo ratings yet
- Modified Vendor Registration Form PDFDocument3 pagesModified Vendor Registration Form PDFAnonymous cKGCdi100% (1)
- Account Details Modification Request FormDocument2 pagesAccount Details Modification Request FormRajkumar manokaranNo ratings yet
- BPCF KCR Placement - Signed ASzDocument5 pagesBPCF KCR Placement - Signed ASzAJay MJNo ratings yet
- Vendor Information Request: Commercial-In-ConfidenceDocument3 pagesVendor Information Request: Commercial-In-Confidencereader131No ratings yet
- Vendor Registration FormDocument2 pagesVendor Registration FormIan SanusiNo ratings yet
- DP & Trading ModificationDocument1 pageDP & Trading ModificationBhalani VijayNo ratings yet
- Renewal NoticeDocument2 pagesRenewal NoticenielNo ratings yet
- Form For Change in Bank Account and Contact DetailsDocument2 pagesForm For Change in Bank Account and Contact DetailsChintan JainNo ratings yet
- Vendor Registration FormDocument15 pagesVendor Registration FormJTO-IT Manipur SSANo ratings yet
- Account Details Addition / Modification Request Form (KRA / Trading / DP A/c)Document1 pageAccount Details Addition / Modification Request Form (KRA / Trading / DP A/c)Pankaj AgarwalNo ratings yet
- Neha Enterprises: Flooring, Dry-Cleaningat (Estb. 2001)Document2 pagesNeha Enterprises: Flooring, Dry-Cleaningat (Estb. 2001)mohitNo ratings yet
- Apply GIRO payments for bills easilyDocument2 pagesApply GIRO payments for bills easilyrachmmmNo ratings yet
- Service Request FormDocument2 pagesService Request FormRS ConsultantsNo ratings yet
- Dua Lima VRF Form NewDocument1 pageDua Lima VRF Form NewOm Sai TravelsNo ratings yet
- CRISIL Group Vendor Registration FormDocument1 pageCRISIL Group Vendor Registration FormrutujaNo ratings yet
- ABL Modification FormDocument1 pageABL Modification FormPochender VajrojNo ratings yet
- Angel Broking Pvt. Ltd. Angel Commodities Broking Pvt. LTDDocument2 pagesAngel Broking Pvt. Ltd. Angel Commodities Broking Pvt. LTDManishSankrityayanNo ratings yet
- Form A1M1Pay1Document19 pagesForm A1M1Pay1arhamdd8No ratings yet
- Aastha Realtors Vendor FormDocument2 pagesAastha Realtors Vendor Formshibani thomasNo ratings yet
- MDBTL Form 20190131220915 7000000081847160Document1 pageMDBTL Form 20190131220915 7000000081847160mohdwajid2009No ratings yet
- IMDA DCA Form PDFDocument1 pageIMDA DCA Form PDFDaps PounchNo ratings yet
- UFlex Mandotry KYC LetterDocument7 pagesUFlex Mandotry KYC Letterabhikumarchoudhary85No ratings yet
- Va 10091Document2 pagesVa 10091Dennis JudsonNo ratings yet
- Metrobank (Updated ATDA Form)Document1 pageMetrobank (Updated ATDA Form)Cherrie Mae CongsonNo ratings yet
- PartialWithdrawalForm 111101697872Document3 pagesPartialWithdrawalForm 111101697872Maheshreddy GNo ratings yet
- Vendor Accreditation FormDocument2 pagesVendor Accreditation Formrowena balaguerNo ratings yet
- Request For Change in Custo Er Details M: Change/Update Contact Details - Residence/Office/Mobile No./ Email IDDocument2 pagesRequest For Change in Custo Er Details M: Change/Update Contact Details - Residence/Office/Mobile No./ Email IDPrakash SinghNo ratings yet
- RM Change Request FormDocument2 pagesRM Change Request FormSk Singh0% (1)
- DDA Form Filling-In GuidelinesDocument5 pagesDDA Form Filling-In GuidelinesfaizalNo ratings yet
- Account details update requestDocument1 pageAccount details update requestvickyNo ratings yet
- Investor Information KitDocument27 pagesInvestor Information KitIyyappadasan SubramanianNo ratings yet
- Vendor Registration Form-Ver2Document1 pageVendor Registration Form-Ver2Anonymous YHmVCTNo ratings yet
- Cleaning and Sweeping Works for RFCL PlantDocument43 pagesCleaning and Sweeping Works for RFCL PlantRameshbabu PeramNo ratings yet
- Customer Maintenance Form ADocument2 pagesCustomer Maintenance Form AWelkin SkyNo ratings yet
- 1 - ENet Application FormDocument6 pages1 - ENet Application FormSahil RajputNo ratings yet
- Standardized Customer Request FormDocument7 pagesStandardized Customer Request FormSimar100% (1)
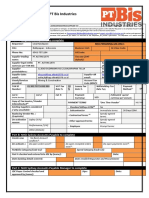
- Supplier Request Form PT Bis Industries: Part A: Originator/Requestor To CompleteDocument3 pagesSupplier Request Form PT Bis Industries: Part A: Originator/Requestor To CompleteOmbONo ratings yet
- AA6376029Document4 pagesAA6376029clientlegalfin2022No ratings yet
- Modified Vendor Registration FormDocument4 pagesModified Vendor Registration Formaman3327No ratings yet
- Standard Operating Procedure for Vendor Master ManagementDocument5 pagesStandard Operating Procedure for Vendor Master ManagementPrateek AgarwalNo ratings yet
- Demat Request Form RetailDocument11 pagesDemat Request Form RetailHarsh YadavNo ratings yet
- Rsec CRF FormDocument3 pagesRsec CRF FormSurya Pratap SinghNo ratings yet
- Customer Application FormDocument2 pagesCustomer Application Formartha permataNo ratings yet
- 1639993422 Phic Eps Enrollment FormDocument2 pages1639993422 Phic Eps Enrollment FormSanito BelazonNo ratings yet
- Demat & Trading AOF Individuals Updated FATCA & PPDIDocument12 pagesDemat & Trading AOF Individuals Updated FATCA & PPDIds462387No ratings yet
- TTS Application FormDocument3 pagesTTS Application FormAbdul RehmanNo ratings yet
- Vendor Number: Vendor Data To Be Completed by Requestor (TNB Department/Subsidiary)Document4 pagesVendor Number: Vendor Data To Be Completed by Requestor (TNB Department/Subsidiary)Mohd Kahirol NizamNo ratings yet
- RIL Payment Slip DetailsDocument2 pagesRIL Payment Slip DetailsKaushal ChauhanNo ratings yet
- Ugc Vendor Accreditation FormDocument3 pagesUgc Vendor Accreditation Formskillmktg2023No ratings yet
- Full Set Applications BiDocument5 pagesFull Set Applications Biprince1900No ratings yet
- EquityclientdetailDocument50 pagesEquityclientdetaildonravadiNo ratings yet
- Update Bank Details for PayoutsDocument2 pagesUpdate Bank Details for Payoutss.sabapathyNo ratings yet
- Form A PDFDocument2 pagesForm A PDFSundar SethNo ratings yet
- Pankaj Resume 1Document2 pagesPankaj Resume 1Daniel CookNo ratings yet
- Request for PAN Card Changes or CorrectionsDocument7 pagesRequest for PAN Card Changes or CorrectionsNAZE COMPUTERNo ratings yet
- Updated EM Complete Notes 2016Document169 pagesUpdated EM Complete Notes 2016Daniel CookNo ratings yet
- Heinz ContractDocument3 pagesHeinz ContractDaniel CookNo ratings yet
- Request for PAN Card Changes or CorrectionsDocument7 pagesRequest for PAN Card Changes or CorrectionsNAZE COMPUTERNo ratings yet
- Ezaz Embroiders: Upper House, Room No. 1, Ground Floor, Jaikarwadi, Shaikh Misreee RoadDocument4 pagesEzaz Embroiders: Upper House, Room No. 1, Ground Floor, Jaikarwadi, Shaikh Misreee RoadDaniel CookNo ratings yet
- A Comparative Study On The Offerings of Insurance Products Between LICDocument26 pagesA Comparative Study On The Offerings of Insurance Products Between LICk b paliwal91% (22)
- Natural DisasterDocument2 pagesNatural DisasterDaniel CookNo ratings yet
- 11111111Document6 pages11111111Daniel CookNo ratings yet
- Gym & Exercise Academy: 1 Google ReviewDocument1 pageGym & Exercise Academy: 1 Google ReviewDaniel CookNo ratings yet
- Essay On Democracy in IndiaDocument1 pageEssay On Democracy in IndiaDaniel CookNo ratings yet
- Skripsi Tanpa PembahasanDocument99 pagesSkripsi Tanpa PembahasanJohanes ProNo ratings yet
- Bir Ruling Un 041 95Document2 pagesBir Ruling Un 041 95mikmgonzalesNo ratings yet
- 05Document19 pages05Emre TürkmenNo ratings yet
- Chapter 1: Accounting in ActionDocument31 pagesChapter 1: Accounting in ActionMohammed Merajul IslamNo ratings yet
- DSLSBill PDFDocument1 pageDSLSBill PDFUdit jainNo ratings yet
- Budgetary Control - L G ElectonicsDocument86 pagesBudgetary Control - L G ElectonicssaiyuvatechNo ratings yet
- Landowner Owner of The Materials: Provided That The Value of The Land Is NotDocument3 pagesLandowner Owner of The Materials: Provided That The Value of The Land Is NotClark LimNo ratings yet
- Tor PMSC UndipDocument22 pagesTor PMSC UndipSigit Nur WaskitoNo ratings yet
- Review 105 - Day 17 P1: How Much of The Proceeds From The Issuance of Convertible Bonds Should Be Allocated To Equity?Document10 pagesReview 105 - Day 17 P1: How Much of The Proceeds From The Issuance of Convertible Bonds Should Be Allocated To Equity?Pola PolzNo ratings yet
- Supplemental Budget Reso 2023Document2 pagesSupplemental Budget Reso 2023Chin RiosNo ratings yet
- Mitigating Control: 1. General InformationDocument2 pagesMitigating Control: 1. General InformationRavi KumarNo ratings yet
- OECD HRM Profile - FinlandDocument4 pagesOECD HRM Profile - FinlandShurel Marl BuluranNo ratings yet
- Global interstate system and institutionsDocument4 pagesGlobal interstate system and institutionsravelyn bresNo ratings yet
- Philippines-Netherlands Tax Treaty Dividend RulingDocument3 pagesPhilippines-Netherlands Tax Treaty Dividend Rulingnathalie velasquezNo ratings yet
- Principles of Finance: Helmut ElsingerDocument260 pagesPrinciples of Finance: Helmut ElsingernikowawaNo ratings yet
- Marketing - Project CDocument7 pagesMarketing - Project Chaithere123No ratings yet
- Chap 04 and 05 (Mini Case)Document18 pagesChap 04 and 05 (Mini Case)ricky setiawan100% (1)
- Financial Modelling CIA 2Document45 pagesFinancial Modelling CIA 2Saloni Jain 1820343No ratings yet
- Contract DocumentsDocument5 pagesContract DocumentsPaul MachariaNo ratings yet
- Balance SheetDocument32 pagesBalance SheetJanine padronesNo ratings yet
- SC-EBRD OriginalDocument6 pagesSC-EBRD OriginalKorporativac KonsaltingićNo ratings yet
- Final Project-Money MarketDocument60 pagesFinal Project-Money MarketSneha Dubey50% (4)
- Mock Reviewer in Management AccountingDocument6 pagesMock Reviewer in Management AccountingJA VicenteNo ratings yet
- SIFTI - Revised 1Document7 pagesSIFTI - Revised 1Leilani JohnsonNo ratings yet
- 2Q2021 Earnings Press ReleaseDocument12 pages2Q2021 Earnings Press ReleaseMike Diaz-AlbisteguiNo ratings yet
- FIN3102 Fall14 Investments SyllabusDocument5 pagesFIN3102 Fall14 Investments SyllabuscoffeedanceNo ratings yet
- Excel Solutions - CasesDocument25 pagesExcel Solutions - CasesJerry Ramos CasanaNo ratings yet
- Power of Compounding CalculatorDocument5 pagesPower of Compounding CalculatorVinod NairNo ratings yet
- Common Mistake and Exam TipsDocument16 pagesCommon Mistake and Exam TipsNguyễn Hồng NgọcNo ratings yet