Oxfam Briefing Paper
Generic competition,
price and access to
medicines
The case of antiretrovirals in
Uganda
Access to treatment is a key part of national strategies to
combat HIV/AIDS. Antiretrovirals can increase the length and
quality of life, and the productivity of patients. Research in
Uganda shows that poor people will use ARVs if the price is
right and if a delivery system is place. It also shows that the
price of brand-name drugs fell significantly only when generics
entered the market. Generic competition, the use of the public-
health safeguards in the TRIPS Agreement, and urgent funding
for health-service delivery are essential parts of the fight against
HIV/AIDS in developing countries such as Uganda.
Summary
John, a local fisherman near Kampala, has felt much better since he started
antiretroviral therapy. He can work and provide for his family. Johns wife
has also recently been diagnosed with HIV. I do not have the money to pay
for medicines for both of us. If he pays for his wife, his children cannot go
to school and they will not have a future. If he stops taking the ARVs to
enable his wife to be treated, he will die. What will happen to my family? he
asks. Like many others, John says a more affordable price would be around
10 per cent of income. This would allow both John and his wife to access
treatment. John believes that the government should help those in need by
cutting the price of ARVs.
The dramatic decrease in morbidity and mortality seen in industrialised
countries due to the use of antiretroviral therapies has not happened in
developing countries, which account for 90 per cent of global HIV infection.
The principal barrier to these life-saving medicines is their high cost, in the
context of low family incomes and public-health budgets. Out of the 1.5 to 2
million HIV-positive Ugandans, only between 5,000 and 10,000 (0.3 0.5 per
cent) are currently receiving antiretroviral therapy. Most of those on treatment
have to sacrifice other family needs in order to pay. Women tend to go
without when families have to make choices about who gets treatment.
This paper outlines the findings of Oxfam research into the accessibility of
ARV therapy in Uganda since 2000. During that year two important events
improved access to these medicines. First, five drug companies agreed to
reduce the price of some ARVs under a UNAIDS scheme. Second, the Joint
Clinical Research Centre (JCRC), the biggest provider of this therapy in
Uganda, imported low-cost generic ARVs from India.
The studys conclusions are:
The crucial role of generic competition. When generic medicines
entered the market, the price of patented medicines fell dramatically. This
finding reinforces the view that an important determinant of price, and
therefore accessibility of ARVs, is competition from generic medicines:
...we had been promised price cuts since May 2000 and didn't see them
until we started to import generics in October, Cissy Kityo, Research and
Clinic Deputy Director of JCRC.
The need for a systematic tiered pricing mechanism. The difficulties
that Oxfam researchers encountered in obtaining information about the
offer from the five companies reinforces the need for a transparent
system of tiered pricing in developing countries. Generic competition
provides the vital benchmark for low prices.
Poor people can use ARVs if the price is right. Interviews clearly
showed that relatively poor people in low-income countries do buy
medicines for life-threatening diseases, but that they have to make huge
sacrifices to do so. As a result of price cuts and generic importation,
JCRC was able to increase the number of patients treated by ARVs from
962 to 3000.
2 Generic competition, price and access to medicines
The need to maximise the use of TRIPS safeguards and ensure that
public health takes precedence over patent rights. After 2005,
Uganda will no longer be able to import generic versions of newly
patented medicines because generic-producing countries, such as India,
will no longer be allowed to export them. Rich-country trade ministers
committed themselves at Doha in November 2001 to find a solution to
this problem by the end of 2002, but are backsliding on this pledge by
putting forward temporary, impracticable, and highly restrictive solutions.
The urgent need to fund health services to deliver treatment.
Funding health services should go hand-in-hand with massive cuts in
prices. The Global Fund provides opportunities for countries such as
Uganda to deliver comprehensive programmes which include treatment
using ARVs.
Generic competition, price and access to medicines 3
1 Introduction
I feel embarrassed because of my medicines and the burden on my family;
I have to constantly struggle to get the money and keep the family going.
Its a tug of war.
At the beginning of his treatment James, a police officer in Kampala, paid
$247 per month. Now that the price of ARVs has decreased he pays $127,
which accounts for all his income and most of his wifes. She has not been
tested, and the family could not afford her treatment if she needed it.
Uganda is considered a success story in combating HIV/AIDS, due
to its early recognition of the implications of the disease and its
vigorous public-education programme. Yet there are between 1.5 and
2 million Ugandans infected by HIV who need treatment. The
Accelerating Access Initiative (AAI) began in May 2000 with an
agreement between the UN and five pharmaceutical companies to
use price reductions to secure a rapid increase in access to
antiretrovirals (ARVs) in developing countries. However, significant
price reductions were not observed until the importation of generic
ARVs by the Joint Clinical Research Council (JCRC), the major centre
among 14 accredited centres for the delivery of treatment in Uganda.
This paper draws on research by Oxfam in Uganda to understand the
current situation in terms of access to ARVs and to describe the role
generic alternatives to these branded medications have played in
increasing accessibility. The research also reviewed Ugandan patent
laws, including the newly proposed Industrial Property Bill 2002 (IP
Bill). The paper presents an overview of the AAI and price trends, the
affordability of treatment, and its impact on patients lives, followed
by a review of the IP laws and some recommendations.
2 Accelerating Access Initiative (AAI)
My children do not know that I am sick. I want them to go to school, and I
do not want them to know that I can die if I do not have my medicines.
Agnes, a shopkeeper and AIDS widow.
Global public pressure led to a partnership between the UN and five
pharmaceutical companies to make a rapid increase in access to
ARVs in selected developing countries by introducing significant
price reductions. Just before the Durban conference on HIV/AIDS,
which focused on treatment, the five companies announced their
intention to cut the prices of ARVs. Apart from GlaxoSmithKline,
which announced a 90 per cent reduction in price, the other four
4 Generic competition, price and access to medicines
companies (Boehringer Ingelheim, Bristol-Myers Squibb, Merck, and
Hoffman-La Roche) did not specify the level of price cuts.
The cuts were welcome, but prices were still too high. Moreover, the
AAI gave no guidance concerning relations between the
pharmaceutical corporations and developing countries. Companies
negotiated directly with governments on a country-by-country, drug-
by-drug basis. Uganda was the first to sign an agreement.
Competition is what brought prices down. There was an 80-90 per cent
price cut when JCRC brought in generics on an emergency basis.
Programme Advisor for UNAIDS in Uganda.
Although the AAI was signed in May 2000, the most significant
reductions in prices for branded ARVs in Uganda coincided with the
importation of generics from an Indian company (Cipla) by JCRC in
October 2000 (Annex 1).
The introduction of generics led to a fall by December 2000 in the
prices of brand-name medicines to between 22 per cent and 70 per
cent of the May 2000 price. By March 2001 the price of AZT and
abacavir to between 44 per cent and 48 per cent of the September
2000 price respectively. The largest decrease was for D4T, which fell
from US$173 for a monthly dose of 40 mg to US 118 in December
2000, to US$ 23 in February 2001, and then eventually to US$6 in
April 2002 (Annex 2). In November 2000, the price of lamivudine was
almost half what it was a month earlier. The price of Combivir, an
important basic double combination, fell from US$220 in May 2000 to
US$71 in February 2001 32 per cent of its original price.
Given that antiretroviral medicines are prescribed in triple
combination, a decrease in the price of just one of the components
prompts an overall decrease in the price of the cocktail. A
combination of Combivir and efavirenz, both branded drugs, costs
$119 per month. By substituting Combivir with the generic
equivalent (Duovir), the cost decreased to $83 per month. The
monthly cost of the triple cocktail of brand-name stavudine,
lamuvidine, and indinavir is US$114. By replacing the first two drugs
with generic equivalents, this is reduced to US$85 per month.
However, the cheapest triple-ARV cocktail is Triomune a generic
drug imported from India which costs $40 per month. It also has
the added value of combining three drugs patented by different
companies into one medicine, making it easier for patients to comply
with the treatment.1 JCRC estimates that 700 of its patients are
currently taking Triomune.
Generic competition, price and access to medicines 5
3 Impact on access
Over half of our patients would stop treatment if we were unable to import
generics. Dr. Cissy Kityo, Deputy Director of JCRC.
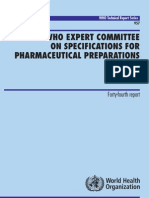
The progressive price cuts were reflected in an increase in the
number of patients receiving ARV therapy at JCRC Centre. With the
importation of generic drugs, JCRC increased the number of patients
on ARV therapy from 962 in 2000 to 3000 in 2001 a 200 per cent
increase in the numbers of patients taking ARVs at one treatment
centre alone. JCRC is the largest provider of ARVs in Uganda,
dispensing roughly 40-70 per cent of all ARVs.
More patients are now accessing treatment beyond the centre,
because JCRC has started providing medicines to some government
regional hospitals. It has already dispensed approximately 2500
doses of generic ARVs, including Triomune, to the Mbarara hospital
between October 2001 and March 2002.
Price reductions also helped patients improve significantly adherence
to their treatment regimen, thus reducing the risk of HIV drug
resistance. However, there is still a long way to go for the thousands
who need the treatment but cannot yet access it.
4 Patents and access to medicines
Seven ARVs are patented in Uganda, five of which have generic
equivalents imported from India. Although these drugs are patented
in Uganda under current IPR law, no lawsuits have yet been filed by
the patent holders. An additional 15 generic ARV registration
applications have been filed with the national drug authority, which
will enhance competition and lower prices.
Under current Ugandan law, patents must be granted for products
and processes for 15 years. Uganda is also a member of the African
Regional Industrial Property Organisation (ARIPO), which has been
frequently used by companies to obtain patents for HIV-related
products. Between 1989 and the end of 2001, 61 ARIPO patent
applications relating to HIV were filed, including the triple-
combination Trizivir.2 The generic equivalent of Trizivir may not be
allowed in Uganda if the patent holder decides to enforce the patent
rights. This would deprive patients of the option of a fixed-dose
combination, which improves adherence.
The Patents Bill 2002 will make Uganda comply with the WTOs
Agreement on Trade Related Aspects of Intellectual Property Rights
6 Generic competition, price and access to medicines
(TRIPS) even before it is obliged to do so. The Agreement requires a
minimum of 20 years patent for new pharmaceutical products and
their processes. If the proposed IP Bill is enacted, not only will
Uganda lose its transition period for TRIPS compliance (until 2006),
but also the further extension until 2016 granted in Doha for
pharmaceutical products.
The TRIPS safeguards, such as compulsory licensing (over-riding a
patent in the public interest) and parallel importing (buying a
patented drug from the cheapest international source), are restricted
under the new Bill. The grounds for compulsory licensing are unclear
and require a judicial process, which opens the door to endless
litigation by companies, and inhibits countries from using this
safeguard. The option of compulsory licensing gives governments a
vital bargaining tool when negotiating lower prices with
pharmaceutical companies.
The Bill also restricts parallel importation to imports by the patent
holder, or with the holder's expressed consent. This will prevent
importation from a third country where the medicine may be on the
market at a much cheaper price.
Over 95 per cent of drugs consumed in Uganda are still imported (33
per cent from India alone), of which 80 per cent are generics.3 Patents
on pharmaceuticals (such as ARVs) can be used to prevent the
importation of cheaper essential medicines and the local manufacture
of similar products.
5 Affordability and funding
Most patients who were interviewed by Oxfam researchers are
spending 50 per cent or more of their monthly incomes on ARVs.
People are making great sacrifices to pay for treatment. The research
found that women with HIV-infected partners are often not tested if
they are not ill, partly because the family could not afford medicines
anyway. It is clear that patients appreciate the value of medicines. I
must continue to pay or I will die, said Charles, a civil servant.
Before I was sick, and now I am fine. In Violets case the treatment
meant that she could work as a shopkeeper, earn money, and send
her children to school.
However, prices are still beyond the means of the majority of patients
who need them. Patients interviewed said that they could pay
around 10 per cent of their income for treatment, and recommended
that the government intervene for further price reductions.
Accredited health centres focus primarily on treating opportunistic
Generic competition, price and access to medicines 7
infections and providing palliative care because the majority of
patients cannot afford ARV therapy.
Why should we tell patients about ARVs when they will not be able
to buy them? It will just make them more depressed. Dr. Moses
Kamya, Co-director Mulago hospital HIV clinic.
Many patients are not aware of generic options available at lower
cost, since the medical profession gets information mainly from the
large pharmaceutical companies promotional material. In addition to
the cost of ARVs, patients have to pay for lab tests. Health centres
must also be equipped, and resources found to pay staff to deliver
treatment services.
6 Conclusion and recommendations
Access to treatment is a crucial element of national strategies to
combat AIDS, and should co-exist with prevention and care. ARVs
can increase the length and quality of life, as well as the productivity
of infected patients, and thus their contribution to the national
economy. Treatment can also offer hope for the future, which is often
a necessary motivation for testing and accepting of safe sex
education. But the high price of medicines is still an impossible
barrier for the very poor, and women are severely disadvantaged in
gaining access to this life-saving treatment.
It was only when generic equivalents to branded drugs entered the
market that the price of brand names came down significantly. This
study showed that, where an organised treatment system was in
place, generic competition led to a 200 per cent increase in the
number of patients using the medicines.
The Ugandan government should ensure that the new IP Bill takes
full advantage of the existing public-health safeguards as confirmed
at Doha, to ensure that Ugandan HIV/AIDS patients can benefit
from the importation of cheap generics in the future.
However, the great majority of HIV-infected Ugandans still cannot
afford to pay for therapy. The international community, especially
the Global Fund to Fight HIV/AIDS, TB, and Malaria, should
support national treatment programmes.
In order to help Ugandan patients to get access to medicines essential
to their survival, donors, the Global Fund, pharmaceutical
companies, and the Ugandan government need to:
Apply a systematic tiered-pricing system whereby developing
countries pay the minimum price of medicines based on the
8 Generic competition, price and access to medicines
marginal cost of production. This will not unduly affect drug
companies profits as these are earned in rich countries. Generic
competition creates price competition, an essential element in
setting the benchmark for low prices.
The Ugandan government should revise the draft Bill to take full
advantage of the public-health safeguards in the TRIPS
Agreement and Doha declaration, including the extra allowable
transition period.
WTO members must agree to an effective solution to the
predicament of countries lacking the capacity to make their own
medicines. Regardless of the TRIPS safeguards, after 2005 they
will have nowhere from which to import them.
The Global Fund should recognise that access to affordable
medicines to combat AIDS includes the delivery of treatment
services. The Fund should support regional and multi-country
bulk purchase of medicines, including generics.
Government and donor programmes should create awareness
among the medical profession and the public regarding the value
of generic medicines.
Generic competition, price and access to medicines 9
Notes
1
Triomune is a combination of generic versions of lamivudine, developed by
GSK, stavudine, developed by Bristol-Myers Squibb, and nevirapine,
developed by Boehringer Ingelheim.
2
A fixed-dose combination of AZT, lamivudine, and abacavir produced by
GSK.
3
National Drug Register, Uganda, December 2001.
Oxfam International 2002 June 2002
This paper was written by Dr. Mohga Kamal Smith, based on research by
Astrid Martinez-Jones and Norbert Anyama, which was co-ordinated in
Uganda by Monica Nagganga and Dereje Wordofa. Oxfam acknowledges
the assistance of Philippa Saunders in its production. It is part of a series of
papers written to inform public debate on development and humanitarian
policy issues. The text may be freely used for the purposes of
campaigning, education, and research, provided that the source is
acknowledged in full.
For further information please email advocacy@oxfaminternational.org
10 Generic competition, price and access to medicines
Im p a c t o f in tr o d u c tio n o f G e n e r ic s o n p r ic e s o f A R V s a n d n u m b e r o f p a tie n t tre a te d
300
N u m b e r o f p a t ie n t s a c c e s s in g A R V s a t
JCRC
4 ,0 0 0
3 ,5 0 0
250 3 ,0 0 0
AZT
2 ,5 0 0
D4T
2 ,0 0 0
ddI
1 ,5 0 0
3TC
200 1 ,0 0 0
A Z T /3 T C
500
N e v ir a p in e
0
96
98
00
02
150
100
50
O c to b e r 2 0 0 0 :
Im p o r t a tio n o f
G e n e r ic s s ta r t s
0
M a y -0 0 A u g -0 0 N o v -0 0 F e b -0 1 M a y -0 1 A u g -0 1 N o v -0 1 F e b -0 2
Generic competition, price and access to medicines 11
Comparison of prices of brand name and generic ARVs in 2002
140
B ra n d c o s t p e r m o n th (U S D )
G e n e ric c o s t p e r m o n th (U S D )
120
100
Price per month in in US $
80
60
40
20
0
A Z T (3 0 0 m g ) D 4 T (4 0 m g ) 3 T C (1 5 0 m g ) AZT+3TC N e v ira p in e (2 0 0 A Z T (3 0 0 m g ) + D 4 T (4 0 m g ) + D 4 T (4 0 m g ) +
(3 0 0 /1 5 0 m g ) m g) 3 T C (1 5 0 m g ) + 3 T C (1 5 0 m g ) + d d I (1 0 0 m g ) +
c o m b iv ir o r d u o v ir N e v ira p in e N e v ira p in e N e v ira p in e
(2 0 0 m g ) (2 0 0 m g ) (2 0 0 m g )
12 Generic competition, price and access to medicines
Chronology of Prices of brand name ARVs
Non-Proprietary Drug Name
May Oct. Nov. 2000 Dec.2000 Dec. Cost as % Jan Feb Jan/Feb cost as Mar April Mar/Apr cost as
2000 May/Sept 2000 2001 % May/Sept 2000 2002 % May/Sept
(Dosage)
2000
NRTIs
Zidovudine/AZT (300 mg) 117 117 117 100% 117 100% 51 44%
Zidovudine/AZT (100 mg) 81 81 81 100% 81 100% 30 37%
Stavudine/D4T (40 mg) 173 118 118 68% 23 13% 6 3%
Stavudine/D4T (20 mg) 160 112 112 70% 15 9% 5 3%
Lamivudine/3TC (150 mg) 98 22 22 22% 22 22% 22 22%
AZT+3TC (300/150 mg) combivir or duovir 220 71 71 32% 71 32% 71 32%
Didanosine/ddI (100 mg) 79 41 41 52% 14 18% 14 18%
Didanosine/ddI (25 mg) 20 10 10 50% 8 40% 8 40%
Abacavir (300 mg) 266 266 266 100% 266 100% 127 48%
NNRTIs
Efavirenz (200 mg) 207 207 103 50% 104 50% 48 23%
Nevirapine (200 mg) 273 137 137 50% 45 16% 45 16%
PIs
Nelfinavir (250 mg) 400 400 400 100% 400 100% 311 78%
Indinavir (400 mg) 289 289 96 33% 96 33% 57 20%
Lopinavir/Ritonavir (133.3/33.3 mg) 62
Generic competition, price and access to medicines 13
Oxfam International is a confederation of twelve development agencies which work in 120
countries throughout the developing world: Oxfam America, Oxfam-in-Belgium, Oxfam
Canada, Oxfam Community Aid Abroad (Australia), Oxfam Germany, Oxfam Great Britain,
Oxfam Hong Kong, Intermn Oxfam (Spain), Oxfam Ireland, Novib, Oxfam New Zealand,
and Oxfam Quebec. Please call or write to any of the agencies for further information.
Oxfam International Advocacy Office, 1112 16th St., NW, Ste. 600, Washington, DC
20036 Tel: 1.202.496.1170, E-mail: advocacy@oxfaminternational.org, www.oxfam.org
Oxfam International Office in Brussels, 60 rue des Quatre Vents, Brussels, B1080
Tel: 322.501.6761
Oxfam International Office in Geneva, 15 rue des Savoises, 1205 Geneva
Tel: 41.22.321.2371
Oxfam International Office in New York, 355 Lexington Avenue, 3rd Floor, New York,
NY 10017 Tel: 1.212.687.2091
Oxfam Germany Oxfam America
Greifswalder Str. 33a 26 West St.
10405 Berlin, Germany Boston, MA 02111-1206
Tel: 49.30.428.50621 Tel: 1.617.482.1211
E-mail: info@oxfam.de E-mail: info@oxfamamerica.org
www.oxfam.de www.oxfamamerica.org
Oxfam-in-Belgium Oxfam Canada
Rue des Quatre Vents 60 Suite 300-294 Albert St.
1080 Burxelles, Belgium Ottawa, Ontario, Canada K1P 6E6
Tel: 32.2.501.6700 Tel: 1.613.237.5236
E-mail: oxfamsol@oxfamsol.be E-mail: enquire@oxfam.ca
www.oxfamsol.be www.oxfam.ca
Oxfam Community Aid Abroad Oxfam Hong Kong
National & Victorian Offices 17/F, China United Centre
156 George St. (Corner Webb Street) 28 Marble Road, North Point
Fitzroy, Victoria, Australia 3065 Hong Kong
Tel: 61.3.9289.9444 Tel: 852.2520.2525
E-mail: enquire@caa.org.au E-Mail: info@oxfam.org.hk
www.caa.org.au www.oxfam.org.hk
Oxfam GB Oxfam Quebec
274 Banbury Road, Oxford 2330 rue Notre-Dame Quest
England OX2 7DZ Bureau 200, Montreal, Quebec
Tel: 44.1865.311.311 Canada H3J 2Y2
E-mail: oxfam@oxfam.org.uk Tel: 1.514.937.1614 www.oxfam.qc.ca
www.oxfam.org.uk E-mail: info@oxfam.qc.ca
Oxfam New Zealand Oxfam Ireland
Level 1, 62 Aitken Terrace 9 Burgh Quay, Dublin 2, Ireland
Kingsland, Auckland, New Zealand 353.1.672.7662 (ph)
PO Box for all Mail: PO Box 68 357 E-mail: oxireland@oxfam.ie
Auckland 1032 52-54 Dublin Road,
New Zealand Belfast BT2 7HN
Tel: 64.9.355.6500 Tel: 44.289.0023.0220
E-mail: oxfam@oxfam.org.nz E-mail: oxfam@oxfamni.org.uk
www.oxfam.org.nz
www.oxfamireland.org
Intermn Oxfam Novib
Roger de Lluria 15 Mauritskade 9
08010, Barcelona, Spain 2514 HD. The Hague, The Netherlands
Tel: 34.93.482.0700 Tel: 31.70.342.1621
E-mail: intermon@intermon.org E-mail: info@novib.nl
www.intermon.org www.novib.nl
Published by Oxfam International July 2002
Published by Oxfam GB for Oxfam International under ISBN 978-1-84814-409-5
14 Generic competition, price and access to medicines
You might also like
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfam100% (1)
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfam100% (2)
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfam100% (1)
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfam100% (1)
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- Gender and Social InclusionDocument28 pagesGender and Social InclusionOxfamNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- (Posco) The Protection of Children From Sexual Offences Act, 2012.Document34 pages(Posco) The Protection of Children From Sexual Offences Act, 2012.anirudha joshiNo ratings yet
- TABLE OF CONTENTS Ewc 661Document5 pagesTABLE OF CONTENTS Ewc 661Abdul QayumNo ratings yet
- STG General HospitalDocument682 pagesSTG General HospitalhaalefomNo ratings yet
- Operasi Bedah Orthopedi 2019Document23 pagesOperasi Bedah Orthopedi 2019DICKY PANDUWINATANo ratings yet
- Final Assignment of TechnologyDocument15 pagesFinal Assignment of TechnologyKazi Mehnaz Subrine 1821385049No ratings yet
- Toplabs Catalog 1Document16 pagesToplabs Catalog 1esteriplasNo ratings yet
- BAMU B.pharmacy Third Year SyllabusDocument48 pagesBAMU B.pharmacy Third Year SyllabusGajanan Vaishnav0% (1)
- The Progress of Radiology in Its First YearDocument53 pagesThe Progress of Radiology in Its First YearHaris HuseinagićNo ratings yet
- Master LBM 1 IntanDocument19 pagesMaster LBM 1 IntanCyntia AndrinaNo ratings yet
- Renal Blood Flow and Its Autoregulation (Seminar)Document39 pagesRenal Blood Flow and Its Autoregulation (Seminar)shival_aiimsNo ratings yet
- Pool Safety BrochureDocument2 pagesPool Safety BrochureKOLD News 13No ratings yet
- Safety Blood Bank By-Dr - Mohamed Barouni 222Document31 pagesSafety Blood Bank By-Dr - Mohamed Barouni 222Hannan AliNo ratings yet
- Ki Oct 23 Kdigo Reco Anemia HifDocument26 pagesKi Oct 23 Kdigo Reco Anemia HifaminaNo ratings yet
- Antihipertenziva Alfa 2 MimeticiDocument10 pagesAntihipertenziva Alfa 2 MimeticiaksymarNo ratings yet
- 21 Gene Breast AssayDocument3 pages21 Gene Breast AssayAnonymous PKE8zOXNo ratings yet
- Applying Philosophy To Science and Technology by Sarah Jane ToledanoDocument24 pagesApplying Philosophy To Science and Technology by Sarah Jane ToledanoNicoelNo ratings yet
- Chapter 10. Human Body System: Respiratory System and Circulatory SystemDocument61 pagesChapter 10. Human Body System: Respiratory System and Circulatory SystemMary Faith BerenguelNo ratings yet
- Delta Fitness: Pelvic Floor 2Document3 pagesDelta Fitness: Pelvic Floor 2Jomari ServanoNo ratings yet
- Pedia Care Study - Appendix B - Drug StudyDocument8 pagesPedia Care Study - Appendix B - Drug Studyryan100% (1)
- The Learners Demonstrate An Understanding ofDocument3 pagesThe Learners Demonstrate An Understanding ofLaira Joy Salvador - ViernesNo ratings yet
- The Longevity Formula of Count Saint GermainDocument9 pagesThe Longevity Formula of Count Saint GermainMiguel Salas-GomezNo ratings yet
- CABALIDA - Herbal PlantsDocument29 pagesCABALIDA - Herbal PlantsJeralyn CABALIDANo ratings yet
- ZK-ZK20 User ManualDocument34 pagesZK-ZK20 User ManualCyberNo ratings yet
- Who TRS 957Document292 pagesWho TRS 957MohamedRefaatMohamedNo ratings yet
- Majority of amino acids used for de novo protein synthesis derives from protein degradation (80Document47 pagesMajority of amino acids used for de novo protein synthesis derives from protein degradation (80Indra ToshiwayNo ratings yet
- MAPEH 10 1st - 100008Document3 pagesMAPEH 10 1st - 100008Punang National High School 309166100% (1)
- Acanthosis NigricansDocument31 pagesAcanthosis NigricansDeval MistryNo ratings yet
- Session 5Document3 pagesSession 5Sistine Rose Labajo100% (1)
- Pola Kehilangan Gigi Dan Kebutuhan Perawatan GigiDocument5 pagesPola Kehilangan Gigi Dan Kebutuhan Perawatan GigiPraprimadani MursyidNo ratings yet
- DRANZCOG Pamphlet Updated 150316Document2 pagesDRANZCOG Pamphlet Updated 150316RGNo ratings yet