Water
A Source of
HOSPITAL Concern for
Infections
by Judy A. Angelbeck, Ph.D.,
Girolamo A. Ortolano, Ph.D.,
Francis P. Canonica, Ph.D.,
and Joseph S. Cervia, M.D.
C
ontamination of the hospital water supply with potentially pathogenic Many waterborne microorganisms
organisms is very common. A wide range of bacteria, fungi, and protozoa are opportunistic pathogens that
in the water supply may be pathogenic and should be cause for clinical can increase the risk of infection in
concern. Common bacterial pathogens include Legionella spp., Pseudomonas immunocompromised patients. Such
aeruginosa, and some mycobacteria. Aspergillus is a particularly disconcerting mold patients who come into contact with
found in hospital water. While the pathogenicity of many waterborne parasites (e.g. contaminated tap water from point-
C ryptosporidium parv u m) has been well documented, some protozoa such as of-use sources such as faucets,
Acanthamoeba are not only pathogenic in their own right, but they can also protect showers, water fountains, and ice
bacterial pathogens such as Legionella pneumophila from destructive chemical machines are therefore challenged with
disinfectants and environmental forces as they support bacterial growth and replication. an increased potential for infection.
Point-of-use water filtration has not
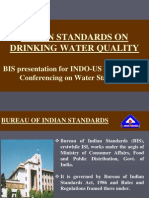
Figure 1 only been shown to reduce infectious
complications, but it also serves as a
complementary strategy to systemic
water disinfection technologies. The
Schematic representation persistence of biofilm in healthcare
of the potential sites of facility water delivery systems provides
waterborne organism further justification for implementing
sequestration within the
point-of-use filtration.
plumbing supply to and
within hospitals. Adapted Overview
from Anaissie et. al.1
In a recent plea for action,
Anaissie et al.1 reviewed the potential
sources of water and mechanisms
through which water could serve as a
source of infectious microorganisms
(Figure 1). A recent extensive review
of topics relevant to waterborne
pathogens also outlines this risk.2
Hospital Water as a Source of
Infectious Microorganisms
Hospitals generally draw their
water from the municipal water
supply. As a consequence of the fact
that municipal water, once disinfected
at the treatment plant, travels through
a system of biofilm-laden pipes
before reaching the hospital, water-
borne microorganisms have been
found in hospital water tanks, as well
44 MANAGING INFECTION CONTROL JANUARY 2006
as the tap water that flows from faucets and showers. It is the Common Waterborne Pathogens
water’s contact with biofilm that is the primary cause of poor Bacteria found in potable water include Legionella pneu -
tap water quality at the point-of-entry to the hospital. However, mophila, Pseudomonas spp. (particularly Pseudomonas
other factors such as distribution pipeline and storage tank age aeruginosa), Stenotrophomonas maltophilia, Aeromonas spp.,
and corrosion, poor water system design, and water stagnation Acinetobacter spp., Enterobacter spp., Flavobacterium spp.,
are also major contributors. Biofilm can become dislodged and Serratia spp. 5,6,7,8,9 P. aeuriginosa can persist in the
from pipe surfaces as the result of increased water demand hospital water supply for extended periods and has been asso-
during the summer months that results in higher water flow ciated with healthcare-associated infection (HAI) outbreaks.1,5
rates and increased shearing forces. Periods during which The bacteria isolated and identified in association with
facility construction takes place also result in biofilm distur- 13 of 17 reported waterborne pathogen outbreaks (76%) were
bance due to direct mechanical contact with pipes, as does the resistant to at least two classes of antibiotics (Table 1; adapted
occasional use of normally stagnant water at less frequently from Anaissie et al.1). A number of reports show that mycobacteria
accessed points-of-use. can be isolated from hospital water. These bacteria can persist in
Patient exposure to waterborne microorganisms in the water systems over several years and have been implicated in
hospital occurs while showering, bathing, drinking water, or HAI outbreaks.10,11,12,13,14,15,16 Among the fungi, Aspergillus
ingesting ice. It can also occur through contact with contami- spores can inhabit hospital water distribution systems. An
nated medical equipment such as tube feed bags, flexible a s p e rgillosis outbreak was reported in a hospital in Houston
endoscopes, and respiratory equipment that have been rinsed leading to patient infections. There is additional evidence that
with tap water. The hands of healthcare personnel washed using other opportunistic molds, including Aspergillus spp., have been
tap water can also lead to patient exposure.1,3,4 recovered from hospital watersystems.17,18,19,20 Among parasites,
Healthcare-associated infections related to contaminated hospital Molecular methods used to establish waterborne microorganisms as
water supplies (tap water and water reservoirs only) with supporting identical to those found infection patients.
molecular relatedness data aligning the contaminating waterborne **Resistant means resistant to two or more clases of antibiotics.
organism to the patient infection.
Table 1A
Organism Source Site(s) of infection Method(s) Used to Link Antibiotic
Patient and Susceptibly
Environmental Strain* of Organism**
BACTERIA
Trautmann et al. 20015 Blood, lungs, peritoneum, AP-PCR Not reported
trachea, urine
Bert et al. 19987 Lung, sinuses, urine DNA macroestriction analysis Resistant
Pseudomonas
Ferroni et al. 19986 Urine PFGE Not reported
aeruginosa
Ezpeleta et al. 199832 Blood ERIC-PCR,RAPD Not reported
Richard et al. 199433 Blood, ling, wound DNA typing, serotyping Resistant
Worlitzsch et al. 198934 Urine ExpoA DNA probe Not reported
Weber et al. 199935 Peritoneum,skin, PFGE Resistant
Stenotrophomonas
respiratory tract,
maltophilia
Talon et al. 199436 Blood, stools, throat, urine PFGE Resistant
Serratia marcescens Carlyn et al. 199837 Eye, stools PFGE Not reported
Acinetobacter Pina et al. 199838 Skin, wound PFGE, biotyping Not reported
baumannii
Aeromonas Picard and Goullet 198739 Blood Electrophoretic esterase typing Not reported
hydrophilia
Chryseobacterium De Schuijmer et al.199840 Blood AP-PCR Not reported
species
46 MANAGING INFECTION CONTROL JANUARY 2006
outbreaks of toxoplasmosis have been reported in municipal deaths per year occur in U.S. hospitals due to waterborne
water supplies and could therefore also potentially reside in healthcare-associated pneumonias caused by Pseudomonas
a hospital water system.21 Finally, while pathogenic viruses aeruginosa alone.
can be recovered from water supplies, no HAIs associated with
waterborne viruses have been reported to date.22
DEFINITION FOR METHOD ABBREVIATIONS USED IN
What is the evidence that healthcare-associated infections TABLE 1 PARTS A, B. AND C.
have been traced to water supplies and/or point-of-use
AP-PCR Arbitrarily Primed Polymerase Chain Reaction
water in the hospital?
Anaissie et al.1 conducted a Medline© search and identified PFGE Pulse-field Gel Electropheresis
43 outbreaks of waterborne healthcare-associated infections ERIC-PCR Enterbacterial Repetitive Intergenic Consensus
for the period 1966-2001. In 29 of the more recent studies
RAPD Random Amplified Polymorphic DNA
where discriminatory methods of strain typing and antibiotic
susceptibility testing were performed, they presented solid ExoA Exotoxin A
evidence that linked the hospital water system to waterborne RFLP Restriction Fragment Length Polymorphism
HAIs in patients (Table 1A, B and C tabulating evidence AFLP Amplified Fragment Length Polymorphism
for water as a source of bacteria, mycobacteria, and fungi
IR-PCR Inter-repeat Polymerase Chain Reaction
that caused infections). Anaissie et al.1 estimated that 1,400
SSDP Sequence Specific DNA Primer Analysis
Table 1B
Organism Source Site(s) of infection Method(s) Used to Link Antibiotic
Patient and Susceptibly of
Environmental Strains Organism**
MYCOBACTERIA
Mycobacterium Von Reyn et al. 199410 Disseminated PFGE Not reported
avium
Kauppinen et al. 199912 Disseminated AP-PCR Susceptible
Mycobacterium
fortuitum Burns et al. 199113 Sputum Phenotype analysis, Partially
plasmid profiles, PFGE reported
Mycobacterium Desplaces et al. 199514 Spine Chromosomal restriction Resistant
xenopi fragment patterns
Mycobacterium Picardeau et al. 199715 Abscess, blood, bone, RFLP, PFGE, AFLP, PCR Not reported
kansasii sputum, stomach, urine
Mycobacterium Sternal wound infection, Resistant to
chelonae prosthetic valve Electrophoresis of enzymes, doxycycline
Wallace et al. 198916 plasmid profiling
Mycobacterium Sternal wound infection Susceptible to
fortuitum doxycycline
Table 1C
Method(s) Used to Link Antibiotic
Organism Source Site(s) of infection Patient and Susceptibly of
Environmental Strains Organism
FUNGI
Fusarium solani Anaissie, 199841 Disseminated RFLP, RAPD, IR-PCR Resistant
Exophiala Nucci et al. 199842 Disseminated RAPD Not reported
jeanselmei
Aspergillus Anaissie et al. 200220 Lungs PCR, SSDP Not reported
fumigatus
JANUARY 2006 MANAGING INFECTION CONTROL 47
Healthcare-associated pneumonias account for Paterson et al.24 tested hot and cold point-of-use water supplies in
20 to 45% of all HAIs and 23,000 deaths per year in 81 transplant units in the UK. As depicted in Figure 2, almost half
the U.S., with 20% of these pneumonias associated (39/81) of the water outlets in these transplant units were found to be
with P. aeruginosa. This suggests that waterborne P. contaminated with Legionella species.
aeruginosa may be a significant contributor to In a recent editorial, Stout et al. identified hospital acquired
healthcare-associated pneumonia in U.S. hospitals.1 Legionnaires’ disease as a global public health issue.25
During a seven-month period, Trautmann et al.5 Key factors influencing the risk of transmission of Legionella include:
observed that 29% (5/17) of patients in a surgical Host susceptibility (immunosuppressed patients such as organ
intensive care unit were infected with P. aeruginosa transplant patients and elderly patients with chronic lung disease).
genotypes that were the same as those detected in the Degree of Legionella colonization within the water supply.
unit’s tap water.
Jarvis et al.23 reported that healthcare-associ- Legionella is a common inhabitant in water distribution systems.
ated bloodstream infections have been traced to In many hospitals, Legionnaires’ disease may go undiagnosed and
water in the operating room environment, with water unrecognized as a cause of patient morbidity and mortality.25 Sabria et
or healthcare workers’ hands playing a critical role in al.26 conducted an environmental surveillance of 20 hospitals in
the contaminating event. Barcelona, Spain. Some of the key findings were:
There are 29 recent studies (Table 1) containing Legionella pneumophial was isolated from 85% (17/20) of the
both epidemiological and molecular relatedness data hospital portable hot water systems.
that incriminate hospital point-of-use tap water and Each hospital had its own unique DNA subtypes of L. pneumophila.
water reservoirs as sources of HAIs in patients. Areas
of the hospital with patient infection outbreaks include: Patients at high risk of infection due to waterborne microorganisms
Surgical Intensive Care Unit include those who are immunocompromised as a consequence of
Neurosurgery Intensive Care Unit their diseases and/or the treatment regimens for their diseases. These include:
Pediatric Oncology Ward AIDS patients
Pediatric Surgical Unit Organ transplant recipients
Cardiovascular Surgery Unit Oncology patients
Burn Unit Neonates
Neonatal Intensive Care Unit Critically ill patients
Figure 2
Contamination of water supply
outlets in transplant units.
Adapted from Patterson et al.24
48 MANAGING INFECTION CONTROL JANUARY 2006
Contaminated water can lead to infection via inhalation of water droplets, Solutions to the Problem of
ingestion of water, immersion in water, or contact with equipment, environ- Contaminated Water
mental surfaces or hands that have been in contact with water.1,25,27,43 Table 2 Can an entire water delivery system be
summarizes several studies which describe the parameters of hospital disease effectively treated to prevent or eradicate
outbreaks traced to water. microbial contamination?
Providing safe water for hospital use
Table 2
provides the obvious benefit of minimizing
Likely
at-risk patient exposure to microbial
Site of pathogens. However, in order to determine
Number of Hospital Site Organism Contaminated
Infection
Patients Water Source whether or not total and complete microbial
eradication from a hospital water supply is
27 Neurosurgery Various P. aeruginosa Water supply7 feasible, it is necessary to understand the
challenges that must be overcome in the
4 Cardiac Sternal Legionella Water used to
Surgery Wound bathe wound43 attempt to attain that goal.
Factors that contribute to the microbial
17 Surgical ICU Blood, lungs, P. aeruginosa Tap water5 contamination of water include:
peritoneum
trachea, urine
The temperature of water at various
points in the water distribution system.
13 Renal Lung Legionella Aerosol The development and persistence of
Transplant from tap44 biofilm in the water delivery system,
particularly in areas of the water distribu-
tion system where water tends to stagnate.
The contamination of medical instruments with waterborne microbes is one The inability of systemic disinfection
potential route of infection that has been extensively discussed. The scientific liter- technologies (e.g. chlorine dioxide, hyper-
ature contains references to patient exposure to waterborne microorganisms through chlorination, copper-silver ionization, hot
contact with contaminated medical equipment (e.g. flexible endoscopes, respiratory water flushing) to reach all locations
equipment, tube feed bags, etc.) that had been rinsed with tap water.1,28,29 within the water delivery system.
The magnitude of the problem caused by waterborne HAIs is largely unrecog- The accumulation of scale in a water
nized. Anaissie et al.1 estimated that healthcare-associated P. aeruginosa delivery system and the role it plays
infections alone are responsible for 1,400 deaths annually in the U.S. While in enhancing the conditions for micro-
Legionella is the best recognized of all waterborne pathogens, and that recogni- bial growth.
tion has led to recommendations for preventing patient exposure that are
L e g i o n e l l a-specific in nature, healthcare-associated waterborne infections by Systemic water disinfection technologies
other microbes such as P. aeruginosa have been largely ignored.1 vary in efficacy and cost.2 Superheated water
Facts to consider include the following: can be used to flush the water delivery system,
Pseudomonas can exist not only in biofilms, but also inside free-living but this method is expensive (e.g. labor to
amoebae. The amoebae that harbor pseudomonads provide a microhabitat perform the operation), potentially dangerous
that protects them from disinfectants.1 (e.g. risk of scalding), and can damage water
Small quantities of bacteria can cause infections.1,19 systems that may not be designed for repeated
Waterborne bacteria may be antibiotic resistant, further complicating treat- high temperature operations.
ment of the HAIs that they cause.1,7,33,35,36,41 Periodic chemical disinfection with
There is a risk of false diagnosis from samples collected by instruments agents such as chlorine, chlorine dioxide
contaminated with waterborne microbes. (ClO2), ozone, and hydrogen peroxide can
Extensive contamination of clinical samples with waterborne microorgan- also be used to reduce the level of microbial
isms can lead to false diagnosis of infection. contamination. However, if used regularly
Fourteen patients were wrongly diagnosed with tuberculosis after contami- at the concentrations recommended, these
nation of bronchoscopes with nontuberculous mycobacteria.30,31 compounds can be corrosive to piping
Several different patients who were initially diagnosed with Legionella failed materials. Although chlorine is routinely
to develop symptoms. Further investigation identified Legionella in the water added to drinking water, many org a n i s m s
supply. Bronchoscopes that had been used in the initial diagnoses were likely are resistant (e.g. Cryptosporidium sp.).
contaminated during the final rinse step of the reprocessing protocol.42 Also, since organic material absorbs
50 MANAGING INFECTION CONTROL JANUARY 2006
chlorine, biocidal activity will be negatively impacted as presence of organic material, high microbial bioburden, and
organic material concentrations increase. Finally, when high turbidity. The effectiveness of UV-generating lamps is
amoeba-resistant bacteria take up residence inside an amoeba also reduced over time by the accumulation of scale, requiring
host that is in turn resistant to a particular chemical disinfectant, maintenance and/or replacement.
they can escape destruction by that disinfectant. Monochloramine (NH2Cl) has been used in certain U.S.
Copper-silver ionization has also been used successfully municipalities to effectively reduce Legionella levels. Concern
in many healthcare facilities. This technology employs an exists, however, regarding its toxic disinfection products.
ionization chamber containing electrodes composed of both Furthermore, there are presently no point-of-entry systems
copper and silver. Electrical current is applied to the electrodes available to deliver monochloramine to individual buildings.
as water passes through the chamber, and copper and silver Systemic water disinfection technologies, although
ions, which have biocidal properties, are released into the water certainly a step in the right direction as relates to the control of
stream. This technology is usually applied only to the hot water waterborne pathogens, vary in their respective abilities to
line and is primarily directed to the control of Legionella sp. effectively respond to changes in water quality that result from
However, failure to address the cold water line leads to seasonal variation, abrupt changes in municipal water system
oversight of the many waterborne organisms that reside in cold pressure, and construction activities within or outside the
water, form biofilm in cold water pipes, and reach the at-risk healthcare facility. In addition, all are incapable of completely
patient in the healthcare setting. and permanently eradicating biofilm that continually exists and
Ultraviolet (UV) radiation is also used systemically, reestablishes itself at downstream locations in the water
but the equipment required is often expensive. Furthermore, delivery system. Finally, they are not maintenance-free and
UV effectiveness is reduced by high water flow, as well as the require periodic attention to maintain peak operating efficiency.
Atlantic Air
AD 1/2 H
Page 51
RS:
JANUARY 2006 MANAGING INFECTION CONTROL 51
Point-of-use filtration complements systemic water by these technologies is not attainable due to the continual
disinfection technologies. establishment of biofilm communities downstream of the
Point-of-use 0.2 micron filters on faucets, showers, water point-of-disinfection. Point-of-use 0.2µm filters present
fountains, and ice machines can reduce the risk of patient and a viable option to provide water for hospital use that
healthcare staff exposure to waterborne pathogens. They can also minimizes patient exposure to waterborne pathogens and
provide a cost effective alternative to the use of bottled water or the risk of waterborne HAIs. While hospital-wide use is
sterile water for drinking by at-risk patients. In hospital units often not required, their application to areas housing
where patient showering and bathing has been restricted for fear patients at highest risk is prudent. Furthermore, in
of waterborne pathogen transmission, point-of-use filters can outbreak situations, the effect of point-of-use filters is
improve patient comfort and quality of life. immediate, and their implementation can mitigate risk
Point-of-use filters complement systemic water disinfection while providing hospital personnel with the appropriate
technologies by trapping free-floating organisms that have survived time to implement a corrective action plan. Finally, with
exposure to disinfectants, broken away from existing biofilm point-of-use filters in place, hospital administration can
colonies located downstream from the point of disinfection, or calmly assess the features and benefits of the various
traveled to the point-of-use from stagnant locations in the water systemic disinfection technology options. ✛
distribution system. Unlike some systemic disinfection technologies
previously described, they also act on both hot and cold water. References
1. Anaissie EJ, Penzak SR, Dignani C. The hospital water supply or a
Point-of-use water filters have been a staple for reducing the
source of nosocomial infection; a plea for action. Arch Intern Med
risk of exposure to waterborne pathogens in healthcare facilities 2002;162:1483-1492.
outside the U.S. for the last 10 years, particularly in Europe. 2. Ortolano GA, McAlister MB, Angelbeck JA, Schaffer J, Russell RL,
However, awareness of their potential benefits is still growing in Maynard E, Wenz B. Hospital Water Point-of-Use Filtration: A
Complementary Strategy to Reduce the Risk of Nosocomial Infection.
the U.S. In light of the broad base of scientific literature that has American Journal of Infection Control 2005; 33(5, Supple 1):S1-S19.
been generated regarding the potential for waterborne pathogens 3. Darelid J, et al. An outbreak of Legionnaires’ Disease in a Swedish
to complicate matters in the care of at-risk patients, as well as the hospital. Scandinavian J Infectious Disease 1994;26:417-425.
4. Marrie TJ et al. Each water outlet is a unique ecological niche for
disease outbreaks traced to waterborne pathogens that are Legoinella pneumophila. Epidemiology Infection 1992;108:261-270.
frequently reported, broad adoption of this technology in the U.S. 5. Trautmann M, Michalsky T, Heidemaire W. Radosavljevic V, Ruhnke
would certainly benefit patients and the healthcare community. M. Tap water colonization with Pseudomonas aeruginosa in a surgical
intensive care unit (ICU) and relation to Pseudomonas infections of
ICU patients. Infect Control Hosp Epidemiol 2001;22:49-52.
Summary 6. Ferroni A, Nguyen B, Pron B, Quesne G, Brusset MC, Berche P.
Contamination of the hospital water supply with potentially Outbreak of nosocomial urinary tract infections due to Pseudomonas
aeru g i n o s ain a pediatric surgical unit associated with tap-water
pathogenic organisms is very common, but the magnitude of the
contamination. J Hosp Infec. 1998;39:301-307.
problem is largely unrecognized, and there are no specific guide- 7. Bert F, Maubec E, Bruneau B, Berry P, Lambert-Zechovsky N. Multi-
lines for protecting patients from exposure. Point-of-use water resistant Pseudomonas aeruginosa outbreak associated with
contaminated tap water in a neurosurgery intensive care unit. J Hosp
(faucets and showers, water fountains, ice machines) may be the
Infect. 1998;39:53-62.
source of the transmission of waterborne microorganisms. Patient 8. Weber DJ, Rutala WA, Blanchet CN, Jordan M, Gergen MF. Faucet
exposure to waterborne pathogens is derived from a number of aerators: a source of patient colonization with Stenotrophomonas
maltophilia.Am J Infect Control. 1999;27:59-63.
sources that include showering, bathing, drinking water, ingestion
9. Carlyn C, Simmonds J, Kondracki S, et al. An outbreak of Serratia
of ice, exposure to contaminated medical equipment that has been marcescens conjunctivitis in a neonatal care unit: genotypic link to an
rinsed with tap water, or the hands of medical personnel washed environmental source. In Program and abstracts of the 8th Annual
and rinsed in tap water. Meeting of the Society for Healthcare Epidemiology of America;
April 5-7, 1998: Orlando, Fla. Abstract 1998: Oral 116.
Ample evidence has now been accumulated to support the 10. Von Reyn C, Maslow JN, Barber TW, Falkinham JO III, Arbeit RD.
presence of waterborne bacteria, fungi, and protozoa in hospital Persistent colonization of potable water as a source of Mycobacterium
water. Molecular relatedness studies have also shown that these avium infection in AIDS. Lancet 1994;343:1137-1141.
11. Soto LE, Bobadilla M, Villalobos Y, et al. Post-surgical nasal cellulites
waterborne organisms are responsible for infections. Certain patient outbreak due to Mycobacterium chelonae. J Hosp Infect. 1991;19:99-106.
populations are at greater risk for infection by waterborne 12. Kauppinen J, Nousiainen T, Jantunen E, Mattila R, Katila ML.
pathogens, namely those who are rendered immunocompromised Hospital water supply as a source of disseminated Mycobacterium
fortuitum infection in a leukemia patient. Infect Control Hosp
either by their disease or by the treatment for their disease (e.g. Epidemiol. 1999;20:343-345.
chemotherapy patients). 13. Burns DN, Wallace RJ, Schultz ME, et al. Nosocomial outbreak
Systemic water disinfection technologies are not completely of respiratory tract colonization with Mycobacterium fort u i t u m:
demonstration of the usefulness of pulsed-field gel electrophoresis in
and sustainably effective in reducing the bioburden of pathogens in an epidemiologic al investigation. Am Rev Respir Dis. 1991;144:
hospitals water. Complete eradication of waterborne microorganisms 1153-1159.
52 MANAGING INFECTION CONTROL JANUARY 2006
14. Desplaces N, Picardeau M, Dinh V, et al. Spinal infections due to 37. Carlyn C, Simmonds J, Kondracki S, et al. An outbreak of Serratia
Mycobacterium xenopi after discectomies. In: Program and abstracts of the marcescens conjunctivitis in a neonatal care unit: genotypic link to an
35th Interscience Conference on Antimicrobial Agents and Chemotherapy: environmental source. In: Program and abstracts of the 8th Annual
September 17-20, 1995; San Francisco, Calif. Abstract J-145. Meeting of the Society for Healthcare Epidemiology of America; April 5-
15. Picardeau M, Prod’Hom G, Raskine L, Le Pennec MP, Vincent V. 7, 1998: Orlando, Fla. Abstract 1998: Oral 116.
Genotypic characterization of five subspecies of Mycobacterium kansasii. 38. Pina P, Guezenec P, Grosbuis S, Guyot L, Ghnassia JC, Allouch PY. An
J Clin Microbiol. 1997;35:25-32. Acinetobacter baumannii outbreak at the Versailies Hospital Center.
16. Wallace RJ, Musser JM, Hull SI, et al. Diversity and sources of rapidly Pathol Biol (Paris), 1998;46:385-394.
growing mycobacteria associated with infections following cardiac 39. Picard B, Goullet P. Epidemiological complexity of hospital Aeromonas
surgery. J Infect Dis. 1989;159:708-716. infections revealed by electrophoretic typing of esterases. Epidemiol
17. Rex JH, Walsh TJ, Anaissie EJ. Fungal infections in iatrogenically Infect. 1987;98:5-14.
compromised hosts. Adv Intern Med. 1998;43:321-371. 40. De Schuijmer J, Vammeste M, Vennecchoutte M, Verschraegen G.
18. Anaissie E, Kuchar R, Rex J, Summerbell R, Walsh T. The hospital water Chryseso bacterium in a burn unit. In: Program and abstracts of the 4th
system as a reservoir of Fusarium. In: Program and abstracts of the 37th International Conference of the Hospitals Infection Society; September
Interscience Conference on Antimicrobial Agents and Chemotherapy; 13-17, 1998; Edinburgh, Scotland.
September 28-October 1, 1997: Toronto, Ontario. Abstract J-94. 41. Anaissie E. Emerging fungi infections: don’t drink the water. In: Program and
19. ter Maaten JC, Golding RP, Strack van Schijndel RJ, Thijs LG. Disseminated abstracts of the 38th Interscience Conference on Antimicrobial Agents and
aspergillosis after near drowning. Neth J Med. 1995;47:21-24. Chemotherapy; September 24-27, 1998; San Diego, Calif. Abstract J-147.
20. Anaissie EJ, Stratton SL, M, Dignani MC, Summerbell RC, Rex JH, 42. Nucci M, Akiti T, Silveira F, et al. Fungemia due to Exophiala jeanselmei:
Monson TP, Spencer T, Kasai M, Francesconi A, Walsh TJ. Pathogenic report of 23 cases. In: Program and Abstracts of the 38th Interscience
Aspergillus species recovered from a hospital water system: A 3-year Conference of Antimicrobial Agents and Chemotherapy; September
Prospective Study. CID 2002;34:780-789. 24-27, 1998; San Diego, Calif. Abstract J-141.
21. Bowie WR, King AS, Werker DH, et al, for the BC Toxoplasma 43. Lowry PW et al. A cluster of Legionella sternal-wound infections due to
Investigation Team. Outbreak of toxoplasmosis associated with municipal postoperative topical exposure to contaminated tap water. New England J
drinking water. Lancet 1997;350:173-177. Medicine 1991;324:109-113.
22. Geldreich EE. Creating microbial quality in drinking water. In: Geldreich 44. Allerberger F, et al. Nosokomiale Legionellen pneumonia bei
EE. Microbial Qualities of Water Supply in Distribution Systems. Boca Nierentranplantieren in Insbruck. Krankenhaus -Hygiene+I nfekt. Verh.
Raton, Fla: CRC Press Inc 1996;39-102. 1993;15:43-47.
23. Jarvis WR, Temprado Cookson S, Robles B. Prevention of Nosocomial
Blood Stream Infections: A National and International Priority. Infection
Control and Hospital Epidemiology 1996;17:272-274.
24. Patterson WJ, et al. Colonization of transplant unit water supplies
with Legionella and protozoa: precautions required to educe the risk of
legonellosis. J Hospital Infect. 1997;37:7-17 and 259-260.
Judy A. Angelbeck, Ph.D., is Senior Vice President of Pall
25. Stout JE, Yu VL. Legionella in the Hospital water supply: a plea for Life Sciences. She has both North American and global medical
decision making based on evidence-based medicine. Infection Control and p roduct experience from more than 22 years in marketing,
Hospital Epidemiology 2001;22:670-672. regulatory and general management. Dr. Angelbeck is currently
26. Sabria M, Garcia-Nunez M, Pedro-Bouel ML, Sopena N, Gimeno JM,
working on development of new products for the somatic cell
Reynaga E, et al. Presence and chromosomal subtyping in potable water
systems in 20 hospitals of Catalonia, Spain. Infect. Control Hosp. therapy market.
Epidemerol 2001;22:673-676. Girolamo A. Ortolano, Ph.D., is Vice President for Scientific
27. Emmerson AM. Emerging Waterborne Infections in Health-Care Settings. Affairs at Pall Corporation. Dr. Ortolano graduated from
Emerging Infectious Disease. 2001;7:272-276. Columbia University (BS) and the University of Rhode Island
28. Dorozynski A. Poor sterilization of instruments leads to infection outbreak
in Paris. British Medical Journal 1997;325-699.
(MS, PhD in Pharmacology), completed a post-doctoral fellow -
29. Mastro TD et al. Nosocomial Legionnaires’ Disease at the use of medication ship at the University of Michigan Hospital, and continued
nebulizers. J Infectious Diseases 1991;163:667-671. research there before joining Pall Corporation. He has authored
30. Gubler JGH, et al. Pseudoepidemic of non-tuberculosus mycobacteria over 90 scientific articles and abstracts including co-authoring
due to a contaminated bronchoscope cleaning machine. Chest 1992;
book chapters.
101:1245-1249.
31. Bennett SN, Peterson DE, Johnson DR, Hall WN, Robinson-Dunn B, Francis P. Canonica, Ph.D., is the Vice President, U.S.
Dietrich S. Am J Respir Crit Care Med. 1994;150:245-250. Healthcare Water Filtration Marketing, at Pall Medical. He has
32. Ezpeleta C, Larrea I, Martinez J, Arrese E, Cisterna R, Pseudomonas more than 25 years of experience in research, product development
aeruginosa bacteremia following ERCP: an investigation of sources by and marketing of medical devices and clinical diagnostics.
molecular typing methods. In: Program and abstracts of the 38th
Interscience Conference on Antimicrobial Agents and Chemotherapy;
Joseph S. Cervia, M.D., is Professor of Clinical Medicine
September 24-27, 1998: San Diego,Calif. Abstract K-73. and Pediatrics at the Albert Einstein College of Medicine in New
33. Richard P, LeFloch R, Chamoux C, Pannier M. Espanze E, Richet H. York and Medical Director and Senior Vice President for Pall
Pseudomonas aeruginosa outbreak in a burn unit: role of antimicrobials in the Corporation. A board-certified internist, pediatrician, adult and
emergences of multiple resistant strains. J Infect Dis. 1994;170:377-383.
pediatric infectious diseases specialist, Dr. Cervia has dedicated
34. Worlitzsch D, Wolz C, Botzenhart K, et al. Molecular epidemiology of
Pseudomonas aeruginosa urinary tract infections in paraplegic patients. much of his career to the care of individuals and families battling
Zentralbl Hyg Umweltmed. 1989;189:175-184. HIV and other infectious diseases, and to clinical re s e a rc h
35. Weber DJ, Rutala WA, Blanchet CN, Jordan M, Gergen MF. Faucet aerators; related to therapeutics, complicating illnesses, and quality of
a source of patient colonization with Stenotrophomonas maltophilia. Am J life issues. He has authored more than 100 articles, chapters
Infec Control 1999;27:59-63.
36. Talon D, Bailly P, Leprat R, et al. Typing of hospital strains of
and abstracts, lectured widely, and serves as a consultant
Xanthomonas maltophilia by pulsed-field gel electrophoresis. J Hosp to numerous local and national organizations on HIV and
Infect. 1994;27:209-217. infectious disease-related issues.
54 MANAGING INFECTION CONTROL JANUARY 2006
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Biotechnology: From Idea To MarketDocument4 pagesBiotechnology: From Idea To MarketTim Sandle100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Cleanroom Contamination Prevention & Control: A Practical Guide To The ScienceDocument13 pagesCleanroom Contamination Prevention & Control: A Practical Guide To The ScienceTim Sandle50% (8)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Conducting Compliant InvestigationsDocument10 pagesConducting Compliant InvestigationsTim Sandle100% (1)
- Publications by Tim SandleDocument62 pagesPublications by Tim SandleTim SandleNo ratings yet
- Digital Transformation in Pharmaceuticals and HealthcareDocument1 pageDigital Transformation in Pharmaceuticals and HealthcareTim Sandle100% (1)
- Publications by Tim Sandle - July 2019Document53 pagesPublications by Tim Sandle - July 2019Tim SandleNo ratings yet
- Microbiological Culture Media: A Complete Guide For Pharmaceutical and Healthcare ManufacturersDocument12 pagesMicrobiological Culture Media: A Complete Guide For Pharmaceutical and Healthcare ManufacturersTim Sandle50% (4)
- Multi Parameter WaterTesting SystemsDocument28 pagesMulti Parameter WaterTesting SystemsAlex SullivanNo ratings yet
- Publications by Tim Sandle - 5th EditionDocument92 pagesPublications by Tim Sandle - 5th EditionTim SandleNo ratings yet
- Can A Bio-Safety Cabinet Be Used As A Fume HoodDocument2 pagesCan A Bio-Safety Cabinet Be Used As A Fume HoodTim SandleNo ratings yet
- Digital Transformation and Regulatory Considerations For Biopharmaceutical and Healthcare Manufacturers Volume 1 Digital Technologies For Automation and Process ImprovementDocument8 pagesDigital Transformation and Regulatory Considerations For Biopharmaceutical and Healthcare Manufacturers Volume 1 Digital Technologies For Automation and Process ImprovementTim SandleNo ratings yet
- Digital Transformation of Pharmaceuticals (New Book)Document2 pagesDigital Transformation of Pharmaceuticals (New Book)Tim SandleNo ratings yet
- NOW IS THE TIME For Animal Welfare in PharmaDocument2 pagesNOW IS THE TIME For Animal Welfare in PharmaTim SandleNo ratings yet
- Dimorph and Filamentous FungiDocument11 pagesDimorph and Filamentous FungiTim SandleNo ratings yet
- Custom Biotech Mycoplasma Pre-Conference WorkshopDocument4 pagesCustom Biotech Mycoplasma Pre-Conference WorkshopTim SandleNo ratings yet
- Recalls Book ContentsDocument15 pagesRecalls Book ContentsTim SandleNo ratings yet
- Pharmaceutical Microbiology NewsletterDocument12 pagesPharmaceutical Microbiology NewsletterTim SandleNo ratings yet
- An Interview With DR Tim Sandle - March 2019Document4 pagesAn Interview With DR Tim Sandle - March 2019Tim Sandle100% (1)
- Cleaning and CleanroomsDocument7 pagesCleaning and CleanroomsTim SandleNo ratings yet
- Robust Quality Audits Are The Solution To Avoiding Expensive RecallsDocument2 pagesRobust Quality Audits Are The Solution To Avoiding Expensive RecallsTim SandleNo ratings yet
- Audit and Control For Healthcare Manufacturers: A Systems-Based ApproachDocument13 pagesAudit and Control For Healthcare Manufacturers: A Systems-Based ApproachTim Sandle100% (1)
- Audit and Control For Healthcare Manufacturers: A Systems-Based ApproachDocument13 pagesAudit and Control For Healthcare Manufacturers: A Systems-Based ApproachTim Sandle100% (1)
- Burkholderia Cepacia Complex: Characteristics, Products Risks and Testing RequirementsDocument17 pagesBurkholderia Cepacia Complex: Characteristics, Products Risks and Testing RequirementsTim Sandle100% (1)
- Biocontamination Control For Pharmaceuticals and HealthcareDocument2 pagesBiocontamination Control For Pharmaceuticals and HealthcareTim Sandle100% (1)
- Real-Time Mycoplasma Contamination Detection For BiomanufacturingDocument3 pagesReal-Time Mycoplasma Contamination Detection For BiomanufacturingTim SandleNo ratings yet
- Artificial Intelligenсe to Improve Cancer Diagnosis in NHSDocument3 pagesArtificial Intelligenсe to Improve Cancer Diagnosis in NHSTim SandleNo ratings yet
- The New Concept of Automatic Gloved Hand SanitizationDocument3 pagesThe New Concept of Automatic Gloved Hand SanitizationTim SandleNo ratings yet
- Pharmigs 26th Annual Conference Programme Interactive 2018 FinalDocument8 pagesPharmigs 26th Annual Conference Programme Interactive 2018 FinalTim SandleNo ratings yet
- Risk Management Library Volume 4: Practical Approaches To Risk Assessment and Management Problem Solving: Tips and Case StudiesDocument6 pagesRisk Management Library Volume 4: Practical Approaches To Risk Assessment and Management Problem Solving: Tips and Case StudiesTim Sandle0% (1)
- Publications by Tim Sandle (3rd Revision)Document42 pagesPublications by Tim Sandle (3rd Revision)Tim SandleNo ratings yet
- Products For Microbiological ControlDocument120 pagesProducts For Microbiological ControlTim Sandle100% (2)
- AR 40-5 Preventive MedicineDocument66 pagesAR 40-5 Preventive MedicineAndrew WilliamsNo ratings yet
- Press Release - Cholera in KampalaDocument2 pagesPress Release - Cholera in KampalaEmma Laura KisaNo ratings yet
- Clean Water and SanitationDocument7 pagesClean Water and SanitationSameeha DorotheaNo ratings yet
- 28-Guidelines For Drinking-Water Quality, Vol. 1, Recommendations (3rd Edition) - WHO-9241546387-Wo PDFDocument541 pages28-Guidelines For Drinking-Water Quality, Vol. 1, Recommendations (3rd Edition) - WHO-9241546387-Wo PDFJai KumarNo ratings yet
- Fowzia Adiyahba PDFDocument86 pagesFowzia Adiyahba PDFGlomarie GonayonNo ratings yet
- BIS - Water Stds PDFDocument45 pagesBIS - Water Stds PDFcsrinivas2100% (1)
- 64e 9Document22 pages64e 9biscaynegroupNo ratings yet
- Analyzing The Implications of Water Privatization: Reorienting The Misplaced DebateDocument38 pagesAnalyzing The Implications of Water Privatization: Reorienting The Misplaced Debateajay thakurNo ratings yet
- Cambodia Water Ver 4-1Document14 pagesCambodia Water Ver 4-1bibintariNo ratings yet
- Hidden ConsequencesDocument80 pagesHidden ConsequencesDanielle DacuanNo ratings yet
- CHN Chapter 13 Environmental Health ADocument38 pagesCHN Chapter 13 Environmental Health AjonaTOTNo ratings yet
- PURCDocument18 pagesPURCDavid James RotamulaNo ratings yet
- IV. Data Presentation, Interpretation and AnalysisDocument43 pagesIV. Data Presentation, Interpretation and AnalysisMaykel JekNo ratings yet
- PVC Pipe Longevity ReportDocument24 pagesPVC Pipe Longevity ReportUnibellNo ratings yet
- Pip 2017 2022 19Document18 pagesPip 2017 2022 19N.a. M. TandayagNo ratings yet
- Moringa Oleifera Seed As Antibacterial Agent in Water TreatmentDocument6 pagesMoringa Oleifera Seed As Antibacterial Agent in Water TreatmentStephen MooreNo ratings yet
- Bhs Putri AyuDocument8 pagesBhs Putri AyuRahmongNo ratings yet
- Sensors 12Document4 pagesSensors 12bassbngNo ratings yet
- Baseline Hygiene KAP Survey HHRD-WASHDocument4 pagesBaseline Hygiene KAP Survey HHRD-WASHSajid KhanNo ratings yet
- Growel Agrovet Private Limited. Products Catalog-EnglishDocument16 pagesGrowel Agrovet Private Limited. Products Catalog-EnglishGrowel Agrovet Private Limited.No ratings yet
- Greenhouse BMP FBDocument152 pagesGreenhouse BMP FBgrNo ratings yet
- 1 s2.0 S0048969722084431 Main 1Document14 pages1 s2.0 S0048969722084431 Main 1Ram PrasathNo ratings yet
- WSWM - Volume 2Document126 pagesWSWM - Volume 2Abeer Abdullah100% (1)
- Giai Chi Tiet de 420 AnhTHPT QG 2019docDocument5 pagesGiai Chi Tiet de 420 AnhTHPT QG 2019docVũ Như QuỳnhNo ratings yet
- The Clean Water Act Is Leading Our Society To A Pleasant Community To Prosper With LifeDocument2 pagesThe Clean Water Act Is Leading Our Society To A Pleasant Community To Prosper With LifeJemifaye AndalNo ratings yet
- PACA-ANAS - MODULE 2 (Health)Document6 pagesPACA-ANAS - MODULE 2 (Health)Cahril Paca-anasNo ratings yet
- Impact of WASH Interventions During Disease Outbreaks in Humanitarian Emergencies: A Systematic Review ProtocolDocument68 pagesImpact of WASH Interventions During Disease Outbreaks in Humanitarian Emergencies: A Systematic Review ProtocolOxfamNo ratings yet
- Water TanzaniaDocument6 pagesWater TanzaniaElite Cleaning ProductsNo ratings yet
- Drinking Water Fountains: A How To GuideDocument30 pagesDrinking Water Fountains: A How To GuideCatalin MihailescuNo ratings yet