You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Spare Parts Documentation: TD10004553 EN 00Document69 pagesSpare Parts Documentation: TD10004553 EN 00Emon Sharma100% (1)
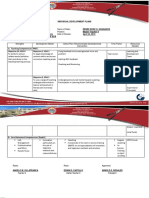
- Individual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Document2 pagesIndividual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Angelo VillafrancaNo ratings yet
- Decolonizing Classrooms - Is There Space For Indigenous Knowledge in A Post-Colonial Society?Document12 pagesDecolonizing Classrooms - Is There Space For Indigenous Knowledge in A Post-Colonial Society?Ahmad HasanNo ratings yet
- Technical Analysis CourseDocument51 pagesTechnical Analysis CourseAkshay Chordiya100% (1)
- Tazkira Mujaddid AlfesaniDocument53 pagesTazkira Mujaddid AlfesanisayedNo ratings yet
- KodalyDocument11 pagesKodalySally Di Martino100% (3)
- Intensive Care Fundamentals: František Duška Mo Al-Haddad Maurizio Cecconi EditorsDocument278 pagesIntensive Care Fundamentals: František Duška Mo Al-Haddad Maurizio Cecconi EditorsthegridfanNo ratings yet
- DRTA-directed Reading Thinking Activity: M. Truscott Staff Development 9-24-10Document13 pagesDRTA-directed Reading Thinking Activity: M. Truscott Staff Development 9-24-10ehaines24No ratings yet
- Po PCitesDocument81 pagesPo PCitessigit nian prasetyoNo ratings yet
- Jurisprudence Examination (Je) Information Guide: 5029-Reginfo - Je V2015.6.Docx Revised July 30, 2015Document10 pagesJurisprudence Examination (Je) Information Guide: 5029-Reginfo - Je V2015.6.Docx Revised July 30, 2015yasahswi91No ratings yet
- Unit 4 Classical and Keynesian Systems: 4.0 ObjectivesDocument28 pagesUnit 4 Classical and Keynesian Systems: 4.0 ObjectivesHemant KumarNo ratings yet
- Syllabus Tourism Laws CKSCDocument6 pagesSyllabus Tourism Laws CKSCDennis Go50% (2)
- Similarities and Differences Between Theravada and Mahayana BuddhismDocument10 pagesSimilarities and Differences Between Theravada and Mahayana BuddhismANKUR BARUA89% (9)
- MDL ChallanDocument1 pageMDL ChallanPratik V PaliwalNo ratings yet
- Grade 10 - SharmajiDocument8 pagesGrade 10 - Sharmajijuned ansariNo ratings yet
- 1404 1284 PDFDocument150 pages1404 1284 PDFJohannRoaNo ratings yet
- Flokulan Air Limbah PDFDocument21 pagesFlokulan Air Limbah PDFanggunNo ratings yet
- Rehabilitation Major Repair of Permanent Bridges Bariis Br.Document2 pagesRehabilitation Major Repair of Permanent Bridges Bariis Br.John Rheynor MayoNo ratings yet
- 2202 Infantilization Essay - Quinn WilsonDocument11 pages2202 Infantilization Essay - Quinn Wilsonapi-283151250No ratings yet
- Jewellery and ZakatDocument2 pagesJewellery and ZakatTariq A MalikNo ratings yet
- Harry Potter and The Prisoner of Azkaban: Chapter 3-1 Owl PostDocument20 pagesHarry Potter and The Prisoner of Azkaban: Chapter 3-1 Owl PostodfasdNo ratings yet
- Corporation Tax CT41G-DciDocument1 pageCorporation Tax CT41G-DciHenry HarrodNo ratings yet
- Assignment On How To Increase Own Brand Mantras: Submition Date: January 29,2021Document5 pagesAssignment On How To Increase Own Brand Mantras: Submition Date: January 29,2021Ferari DroboNo ratings yet
- Santrock Section 1 Chapter 1Document19 pagesSantrock Section 1 Chapter 1Assumpta Minette Burgos75% (8)
- Student Skeletal System Exam QuestionsDocument3 pagesStudent Skeletal System Exam Questionsawiniemmanuel247No ratings yet
- HG G2 Q1 W57 Module 3 RTPDocument11 pagesHG G2 Q1 W57 Module 3 RTPJennilyn Amable Democrito100% (1)
- ch27 Matrices and ApplicationsDocument34 pagesch27 Matrices and Applicationschowa fellonNo ratings yet
- Suspension Mansons 2Document45 pagesSuspension Mansons 2Andres Silva67% (3)
- Comparative DegreeDocument25 pagesComparative DegreeAgung PriyanaNo ratings yet
- Technical Activities: Ken Goldberg, VP Technical Activities Spring 2007, ICRA, RomeDocument52 pagesTechnical Activities: Ken Goldberg, VP Technical Activities Spring 2007, ICRA, RomeWasim Ahmad KhanNo ratings yet