You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Psychological TestingDocument149 pagesPsychological Testingcadpsy100% (16)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Nursing AdministrationDocument64 pagesNursing Administrationjosephsantuyo0% (1)
- Mapua Thesis Format 2020Document12 pagesMapua Thesis Format 2020Synchelle CarmeloNo ratings yet
- Morecambe Marina Feasibility Study Main Report PDFDocument59 pagesMorecambe Marina Feasibility Study Main Report PDFharyanto99100% (1)
- Mathematics: Quarter 4 - Module 3 Interpreting Measures of PositionDocument14 pagesMathematics: Quarter 4 - Module 3 Interpreting Measures of PositionDianne Dynah Bilaro Dy100% (3)
- High Quality Relationships Psychological Safety - Learning From Failures in Work OrganizationsDocument21 pagesHigh Quality Relationships Psychological Safety - Learning From Failures in Work OrganizationsIacopo NicelliNo ratings yet
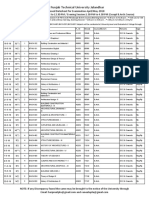
- Prposed Date Sheet Upload Web SiteDocument154 pagesPrposed Date Sheet Upload Web SiteShaheer ShafatNo ratings yet
- Ch22 Managing A Holistic Marketing OrganizationDocument2 pagesCh22 Managing A Holistic Marketing OrganizationRina Fordan Bilog100% (1)
- Network Analysis of The Stock Market: Wenyue Sun, Chuan Tian, Guang YangDocument8 pagesNetwork Analysis of The Stock Market: Wenyue Sun, Chuan Tian, Guang Yangayushi kNo ratings yet
- Awareness and Perception of HousewivesDocument9 pagesAwareness and Perception of HousewivesChrislyn CalinggalNo ratings yet
- BT 406 M.C.Q File by Amaan KhanDocument37 pagesBT 406 M.C.Q File by Amaan KhanMuhammad TahirNo ratings yet
- Operations Research - BMS - AssignmentDocument1 pageOperations Research - BMS - AssignmentJennifer MathaisNo ratings yet
- 008fnh Bacani FTDocument6 pages008fnh Bacani FTmauliana maul100% (1)
- ACCA Qualification Global BrochureDocument22 pagesACCA Qualification Global BrochurejwjzNo ratings yet
- hm5 2015Document2 pageshm5 2015Mickey WongNo ratings yet
- Communicating Authentic Assessment ResultsDocument14 pagesCommunicating Authentic Assessment ResultsGlennson Loyola100% (1)
- Cost Estimation: AACSB: AnalyticDocument30 pagesCost Estimation: AACSB: AnalyticMaryane AngelaNo ratings yet
- How Organizational Culture Shapes CompetitiveDocument14 pagesHow Organizational Culture Shapes CompetitiveHao Wu100% (1)
- Chapter1 Introduction2Document71 pagesChapter1 Introduction2mohammadsaim767No ratings yet
- Veterinary Pharmacy, A Dismissed Necessity PDFDocument3 pagesVeterinary Pharmacy, A Dismissed Necessity PDFKelma TayebaNo ratings yet
- Syllabus: Summary of Information On Each Course: Final Year Project IiDocument9 pagesSyllabus: Summary of Information On Each Course: Final Year Project IiHAZWANI BT SAPAR MoeNo ratings yet
- Effects of Online Learning Mode in Psychological Aspect of College StudentsDocument4 pagesEffects of Online Learning Mode in Psychological Aspect of College StudentsChrizel DiamanteNo ratings yet
- SodaPDF Converted SankhyikiDocument2 pagesSodaPDF Converted SankhyikiAnshika MehtaNo ratings yet
- Assignment 01 SolutionDocument5 pagesAssignment 01 SolutionNeven Ahmed HassanNo ratings yet
- Discovery Approach: Creating Memorable LessonsDocument4 pagesDiscovery Approach: Creating Memorable LessonsAljo Cabos GawNo ratings yet
- Barkway2001. Michael Crotty and Nursing PhenomenologyDocument5 pagesBarkway2001. Michael Crotty and Nursing PhenomenologymalextomasNo ratings yet
- Visual CognitionDocument34 pagesVisual CognitionjacqgarsanNo ratings yet
- Tensegrity Based Morphing Structures: Project ReportDocument15 pagesTensegrity Based Morphing Structures: Project ReportKenechukwu OkoyeNo ratings yet
- Environmental PsychologyDocument5 pagesEnvironmental PsychologybevmoczNo ratings yet
- (Lecture Notes in Logistics) Ana Paula Barbosa Póvoa, Albert Corominas, João Luís de Miranda (Eds.)-Optimization and Decision Support Systems for Supply Chains-Springer International Publishing (2017)Document198 pages(Lecture Notes in Logistics) Ana Paula Barbosa Póvoa, Albert Corominas, João Luís de Miranda (Eds.)-Optimization and Decision Support Systems for Supply Chains-Springer International Publishing (2017)Lamchochiya MahaanNo ratings yet