You might also like
- KL Approach Pelvic Course 2013Document31 pagesKL Approach Pelvic Course 2013CepreanNo ratings yet
- 9hOzKCurs DiabetDocument202 pages9hOzKCurs DiabetCepreanNo ratings yet
- Diagnostic Colita Clostridium DifficileDocument21 pagesDiagnostic Colita Clostridium DifficileCepreanNo ratings yet
- Progression of HCV Over Time (Several Decades) : End Stage Liver Disease Hepatocellular CarcinomaDocument7 pagesProgression of HCV Over Time (Several Decades) : End Stage Liver Disease Hepatocellular CarcinomaCepreanNo ratings yet
- ContentsDocument1 pageContentsPavel SebastianNo ratings yet
- Encefalopatia Hepatica MinimaDocument7 pagesEncefalopatia Hepatica MinimaCepreanNo ratings yet
- CV Template Europass (English)Document2 pagesCV Template Europass (English)jobiehelpNo ratings yet
- Log FileDocument1 pageLog FileCiprian CercelNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Constitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofDocument10 pagesConstitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofRichard ObinwankwoNo ratings yet
- Chest TraumaDocument47 pagesChest Traumafrenee aradanasNo ratings yet
- Arrow Wounds and Treatments On The Western FrontierDocument7 pagesArrow Wounds and Treatments On The Western FrontierbravofNo ratings yet
- The Axial Skeleton PDFDocument9 pagesThe Axial Skeleton PDFElvin EzuanNo ratings yet
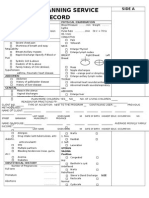
- Family Planning Service RecordDocument3 pagesFamily Planning Service RecordRJay Mon Marcos100% (2)
- Assesment Trauma PatientDocument10 pagesAssesment Trauma PatientCahyani KurniaNo ratings yet
- RLE-level-2-packet-week-12-requirement (SANAANI, NUR-FATIMA, M.)Document26 pagesRLE-level-2-packet-week-12-requirement (SANAANI, NUR-FATIMA, M.)Nur SanaaniNo ratings yet
- Respiratory ENT Assessment GuideDocument3 pagesRespiratory ENT Assessment GuidepriyaNo ratings yet
- Human Respiratory System NotesDocument11 pagesHuman Respiratory System NotesVishal SharmaNo ratings yet
- TEST BANK Chapter 21Document6 pagesTEST BANK Chapter 21Louise Lorraine TaculodNo ratings yet
- BODYBALANCE 96 Choreography Booklet (Spanish)Document34 pagesBODYBALANCE 96 Choreography Booklet (Spanish)leonardo neiraNo ratings yet
- Breathing Exercises: Breathing As A BridgeDocument8 pagesBreathing Exercises: Breathing As A BridgeMilan ValachovicNo ratings yet
- 07 Post Mortem Examination (Autopsy)Document48 pages07 Post Mortem Examination (Autopsy)ARIF-UR-REHMAN100% (5)
- Pa2 and Pa3 2Document14 pagesPa2 and Pa3 2Roger ViloNo ratings yet
- 2013DRAFTMEMSProtocols062713 PDFDocument134 pages2013DRAFTMEMSProtocols062713 PDFMarian Ioan-LucianNo ratings yet
- Grounding ExerciseDocument4 pagesGrounding ExercisecrystalNo ratings yet
- Temporal Sphenoidal Line T2Document3 pagesTemporal Sphenoidal Line T2taichi7No ratings yet
- MR 20-12-14Document131 pagesMR 20-12-14Firdha RositaNo ratings yet
- Denver Yoga Ebook Guide for Home PracticeDocument55 pagesDenver Yoga Ebook Guide for Home PracticeSuosuo Lo0% (1)
- Anatomy Workbook ThoraxDocument68 pagesAnatomy Workbook ThoraxClara AtiyehNo ratings yet
- 3.1 Fixation by Perfusion PDFDocument2 pages3.1 Fixation by Perfusion PDFZul AzmiNo ratings yet
- Speech and Hearing Science-Anotomy and Physiology ZemlinDocument622 pagesSpeech and Hearing Science-Anotomy and Physiology ZemlinelkkrotNo ratings yet
- Microsoft Word - Bk1-LESSONS 1Document78 pagesMicrosoft Word - Bk1-LESSONS 1Dali Soares De Sá NardeliNo ratings yet
- Vats Yustinus Rurie WirawanDocument6 pagesVats Yustinus Rurie Wirawanrurie wirawanNo ratings yet
- Phytochemical Analysis in Capsicum SPP.: March 2016Document154 pagesPhytochemical Analysis in Capsicum SPP.: March 2016AbdurrohimnNo ratings yet
- Health Assessment FinalsDocument25 pagesHealth Assessment FinalserythromycinNo ratings yet
- Lec 1 Gangrene: C. Upper Extremities Are More Commonly Involved Than Lower ExtremitiesDocument13 pagesLec 1 Gangrene: C. Upper Extremities Are More Commonly Involved Than Lower ExtremitiesarbazNo ratings yet
- Health Assessment On Asthma ANPDocument7 pagesHealth Assessment On Asthma ANPSam TullyNo ratings yet
- Assessment of Thorax and LungsDocument15 pagesAssessment of Thorax and LungsmakathrinasanchezNo ratings yet
- CT/MRI Ordering Guide: Body Part Signs/Symptoms Exam To OrderDocument2 pagesCT/MRI Ordering Guide: Body Part Signs/Symptoms Exam To OrderCourtNo ratings yet