You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Sample Discharge SummaryDocument4 pagesSample Discharge SummaryPatient Safety My100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Improving Adherence in Cardiovascular Care ToolkitDocument152 pagesImproving Adherence in Cardiovascular Care ToolkitDenis MiokovićNo ratings yet
- Content 886 PDFDocument2 pagesContent 886 PDFSuci NudiNo ratings yet
- Syphilis Nursing ManagementDocument2 pagesSyphilis Nursing ManagementLizaEllaga67% (3)
- Public Sector Marketing Importance and CharacteristicsDocument7 pagesPublic Sector Marketing Importance and CharacteristicsIJEPT Journal100% (1)
- Ant7 Falls 630 - FULL PDFDocument13 pagesAnt7 Falls 630 - FULL PDFIonela TomescuNo ratings yet
- Adam PharmaDocument18 pagesAdam PharmawaelajlanyNo ratings yet
- The Hospital TeamDocument23 pagesThe Hospital TeamOptimistic Smile67% (3)
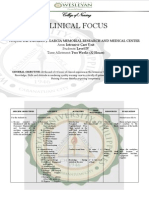
- Clinical Focus ICUDocument6 pagesClinical Focus ICUJan Rainier Carlos BalariaNo ratings yet
- E-Portfolio - Course Reflection 14 MHDocument1 pageE-Portfolio - Course Reflection 14 MHapi-353669394No ratings yet
- E-Portfolio - Course Reflection 16 TransitionsDocument1 pageE-Portfolio - Course Reflection 16 Transitionsapi-353669394No ratings yet
- E-Portfolio - Course Reflection 15 CapstoneDocument1 pageE-Portfolio - Course Reflection 15 Capstoneapi-353669394No ratings yet
- E-Portfolio - Course Reflection 13 Community 2Document1 pageE-Portfolio - Course Reflection 13 Community 2api-353669394No ratings yet
- E-Portfolio - Course Reflection 11 PedsDocument1 pageE-Portfolio - Course Reflection 11 Pedsapi-353669394No ratings yet
- E-Portfolio - Course Reflection 12 CCDocument1 pageE-Portfolio - Course Reflection 12 CCapi-353669394No ratings yet
- E-Portfolio - Course Reflection 10 ObDocument1 pageE-Portfolio - Course Reflection 10 Obapi-353669394No ratings yet
- E-Portfolio - Course Reflection 4 PharmDocument1 pageE-Portfolio - Course Reflection 4 Pharmapi-353669394No ratings yet
- Letter To The Editor Final - William ErskineDocument2 pagesLetter To The Editor Final - William Erskineapi-353669394No ratings yet
- E-Portfolio - Course Reflection 9 Nursing ResearchDocument1 pageE-Portfolio - Course Reflection 9 Nursing Researchapi-353669394No ratings yet
- E-Portfolio - Course Reflection 6 Nursing in CommunityDocument1 pageE-Portfolio - Course Reflection 6 Nursing in Communityapi-353669394No ratings yet
- E-Portfolio - Course Reflection 7Document2 pagesE-Portfolio - Course Reflection 7api-353669394No ratings yet
- E-Portfolio - Course Reflection 8 Prof 3Document1 pageE-Portfolio - Course Reflection 8 Prof 3api-353669394No ratings yet
- E-Portfolio - Course Reflection 2 Health AssessmentDocument1 pageE-Portfolio - Course Reflection 2 Health Assessmentapi-353669394No ratings yet
- E-Portfolio - Course Reflection 5 Professional Nursing 1Document1 pageE-Portfolio - Course Reflection 5 Professional Nursing 1api-353669394No ratings yet
- E-Portfolio - Course Reflection 3 PathophysiologyDocument1 pageE-Portfolio - Course Reflection 3 Pathophysiologyapi-353669394No ratings yet
- Complex Care Concept MapDocument6 pagesComplex Care Concept Mapapi-353669394No ratings yet
- Research PaperDocument10 pagesResearch Paperapi-345759649No ratings yet
- Mental Health - Case StudyDocument11 pagesMental Health - Case Studyapi-353669394No ratings yet
- E-Portfolio - Course Reflection 1 Contemp NursingDocument1 pageE-Portfolio - Course Reflection 1 Contemp Nursingapi-353669394No ratings yet
- E-Portfolio - Philosophy of NursingDocument2 pagesE-Portfolio - Philosophy of Nursingapi-353669394No ratings yet
- Nursing Transitions ResumeDocument1 pageNursing Transitions Resumeapi-353669394No ratings yet
- E-Portfolio - Letter of PresentationDocument2 pagesE-Portfolio - Letter of Presentationapi-353669394No ratings yet
- Weebly - E-Portfolio DescriptionDocument1 pageWeebly - E-Portfolio Descriptionapi-353669394No ratings yet
- Context Diagram Online Enrollment SystemDocument1 pageContext Diagram Online Enrollment SystemRandy Lamarca Alabab0% (1)
- Physical Activ HRQOLDocument7 pagesPhysical Activ HRQOLIulia PaşcalăuNo ratings yet
- Collaborative Care Plan DyspneaDocument6 pagesCollaborative Care Plan DyspneaSara MoreiraNo ratings yet
- Information Technology System Applicable To Nursing PracticeDocument56 pagesInformation Technology System Applicable To Nursing PracticeKristle Ann VillarealNo ratings yet
- Norcet Result 2022Document333 pagesNorcet Result 2022Alapan KarNo ratings yet
- Children's Miracle Network Presents Capital GrantsDocument3 pagesChildren's Miracle Network Presents Capital GrantsNewzjunkyNo ratings yet
- HKGC Booklet FinalDocument95 pagesHKGC Booklet FinalAtik Badshah SHAIKHNo ratings yet
- RCDSO Standard of Practice IPACDocument40 pagesRCDSO Standard of Practice IPACKartikay SrivastavaNo ratings yet
- Jean WatsonDocument2 pagesJean WatsonShanilyn Biong0% (1)
- HM 205 Hospital and Health System 2 2010Document4 pagesHM 205 Hospital and Health System 2 2010Madhurima ChakrabortyNo ratings yet
- Core CompetenciesDocument3 pagesCore Competenciesapi-521620733No ratings yet
- Salva Nursing InfoDocument3 pagesSalva Nursing InfoJohn Leo R. GradoNo ratings yet
- 3 Sujets Science 1 Et 2Document4 pages3 Sujets Science 1 Et 2RihabSallamNo ratings yet
- Rastriya Bal Swasthya KaryakaramDocument3 pagesRastriya Bal Swasthya KaryakaramSachin ParmarNo ratings yet
- Understanding The Labour Market of Human Resources For Health in CameroonDocument27 pagesUnderstanding The Labour Market of Human Resources For Health in CameroonIsmael DkNo ratings yet
- ID Analisis Kesiapan Asosiasi Pengobat Tradisional Terhadap Rencana Implementasi PeDocument11 pagesID Analisis Kesiapan Asosiasi Pengobat Tradisional Terhadap Rencana Implementasi PeTpoad P-AspetriNo ratings yet
- English 2am18 Rattr1Document2 pagesEnglish 2am18 Rattr1Sara AliNo ratings yet
- For PrintDocument17 pagesFor Printexample mailNo ratings yet
- 146336-Article Text-386661-1-10-20161019Document8 pages146336-Article Text-386661-1-10-20161019Huri AbbasiNo ratings yet
- 20-TRICARE Young Adult Info SheetDocument4 pages20-TRICARE Young Adult Info Sheetdnique1985No ratings yet
- Assignment Title: TC1 Response To A Live Employer BriefDocument16 pagesAssignment Title: TC1 Response To A Live Employer Briefsyeda maryemNo ratings yet