HEMATOCRIT/HCT AND
CALCULATED HEMOGLOBIN/HB
Hematocrit is determined conductometrically. The measured conductivity, after correction for electrolyte
concentration, is inversely related to the hematocrit.
See below for information on factors affecting results. Certain substances, such as drugs, may affect analyte
levels in vivo.1
If results appear inconsistent with the clinical assessment, the patient sample should be retested using
another cartridge.
Intended Use
The test for hematocrit, as part of the i-STAT System, is intended for use in the in vitro quantification of
packed red blood cell volume fraction in arterial, venous, or capillary whole blood.
Hematocrit measurements can aid in the determination and monitoring of normal or abnormal total red
cell volume status including, but not limited to, conditions such as anemia, erythrocytosis, and blood loss
related to trauma and surgery.
Contents
Each i-STAT cartridge contains one reference electrode (when potentiometric sensors are included in the
cartridge configuration), sensors for the measurement of specific analytes, and a buffered aqueous calibrant
solution of known conductance that contains known concentrations of analytes and preservatives.
Metrological Traceability
The iSTAT System test for hematocrit measures packed red blood cell volume fraction in arterial, venous,
or capillary whole blood (expressed as the % packed cell volume) for in vitro diagnostic use. Hematocrit
values assigned to iSTATs working calibrators are traceable to the Clinical and Laboratory Standards
Institute (CLSI) H7-A3 procedure for determining packed cell volume by the microhematocrit method.2
Further information regarding metrological traceability is available from Abbott Point of Care Inc.
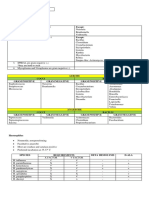
Expected Values
Reportable Reference
Test/Abbreviation Units* Range Range3
Hematocrit/Hct %PCV 10 75 38 51**
Fraction 0.10 0.75 0.38 0.51
Hemoglobin/Hb g/dL 3.4 25.5 12 17
g/L 34 255 120 170
mmol/L 2.1 15.8 7 11
* The i-STAT System can be configured with the preferred units.
**The reference ranges for hematocrit and hemoglobin span both female and male populations.
Rev. Date: 12-Feb-14 Art: 714178-00P
To convert a result from %PCV to fraction packed cell volume, divide the %PCV result by 100. For the
measurement of hematocrit, the i-STAT System can be customized to agree with methods calibrated by
the microhematocrit reference method using either K3EDTA or K2EDTA anticoagulant. Mean cell volumes
of K3EDTA anticoagulated blood are approximately 2-4% less than K2EDTA anticoagulated blood.2 While
the choice of anticoagulant affects the microhematocrit method to which all hematocrit methods are
calibrated, results from routine samples on hematology analyzers are independent of the anticoagulant
used. Since most clinical hematology analyzers are calibrated by the microhematocrit method using K3EDTA
anticoagulant, the i-STAT System default customization is K3EDTA.
The reference range programmed into the analyzer and shown above is intended to be used as a guide
for the interpretation of results. Since reference ranges may vary with demographic factors such as
age, gender and heritage, it is recommended that reference ranges be determined for the population
being tested.
Clinical Significance
Hematocrit is a measurement of the fractional volume of red blood cells. This is a key indicator of the
bodys state of hydration, anemia or severe blood loss, as well as the bloods ability to transport oxygen.
A decreased hematocrit can be due to either overhydration, which increases the plasma volume, or a
decrease in the number of red blood cells caused by anemias or blood loss. An increased hematocrit can be
due to loss of fluids, such as in dehydration, diuretic therapy, and burns, or an increase in red blood cells,
such as in cardiovascular and renal disorders, polycythemia vera, and impaired ventilation.
Performance Characteristics
The typical performance data summarized below were collected in health care facilities by health care
professionals trained in the use of the i-STAT System and comparative methods.
Precision data were collected in multiple sites as follows: Duplicates of each control fluid were tested in the
morning and in the afternoon on five days for a total of 20 replicates. The averaged statistics are presented
below.
Method comparison data were collected using CLSI guideline EP9-A4. Venous blood samples, collected in
lithium heparin Vacutainer tubes, were analyzed in duplicate on the i-STAT System and on the comparative
methods for hematocrit within 20 minutes of collection.
Deming regression analysis5 was performed on the first replicate of each sample. In the method comparison
table, n is the number of specimens in the data set, Sxx and Syy refer to estimates of imprecision based
on the duplicates of the comparative and the i-STAT methods respectively, Sy.x is the standard error of the
estimate, and r is the correlation coefficient.*
Method comparisons will vary from site to site due to differences in sample handling, comparative method
calibration and other site specific variables.
Interference studies were based on CLSI guideline EP7-P.6
*The usual warning relating to the use of regression analysis is summarized here as a reminder: For any analyte, if the data is collected over a narrow
range, the estimate of the regression parameters are relatively imprecise and may be biased. Therefore, predictions made from these estimates may be
invalid.5 The correlation coefficient, r, can be used as a guide to assess the adequacy of the comparative method range in overcoming this problem.
As a guide, the range of data can be considered adequate if r>0.975.
Precision Data (%PCV)
Whole Blood Control Mean SD %CV
Low 30.0 0.44 1.5
High 49.0 0.50 1.0
Hct - 2 Art: 714178-00P Rev. Date: 12-Feb-14
Method Comparison (%PCV)
Coulter S Plus Nova STAT Profile Abbott Sysmex SE9500
5 Cell-Dyn 4000
n 142 192 29 29
Sxx 0.50 0.46 0.41 0.53
Syy 1.09 1.31 0.77 0.76
Slope 0.98 1.06 1.06 1.11
Intt 1.78 -3.98 -1.42 -4.19
Sy.x 2.03 2.063 1.13 0.98
Xmin 18 21 19 24
Xmax 51 50 46 47
r 0.952 0.932 0.993 0.980
Factors Affecting Results*
The measurement of certain blood samples with high erythrocyte sedimentation rates (ESR) may be
affected by analyzer angle. While testing blood samples, beginning ninety (90) seconds after the cartridge
is inserted, the analyzer should remain level until a result is obtained. A level surface includes running the
handheld in the downloader/recharger.
Interferent Effect
WBC Grossly elevated white blood cell counts may increase results.
Total Protein Hematocrit results are affected by the level of total protein as follows:
Displayed Result TP < 6.5 g/dL TP > 8.0 g/dL
HCT < 40 %PCV Hct decreased by ~1% PCV Hct increased by ~1% PCV
for each decrease of for each increase
1 g/dL TP 1 g/dL TP
HCT > 40 % PCV Hct decreased by ~0.75 % PCV Hct increased by ~0.75 %PCV
for each decrease of for each increase
1 g/dL TP 1 g/dL TP
Total protein levels may be low in neonatal and burn patient populations, as well
as in additional clinical populations listed in Statland.3 Total protein levels may also
be decreased in patients undergoing cardiopulmonary bypass (CPB) or ECMO,
and with patients receiving large volumes of saline-based IV fluids. Care should be
taken when using hematocrit results from patients with total protein levels below
the adult reference range (6.5 to 8 g/dL).
The CPB sample type can be used to correct the hematocrit result for the dilutional
affect of the pump prime in cardiovascular surgery. The CPB algorithm assumes
that cells and plasma are diluted equally and that the pump priming solution has
no added albumin or other colloid or packed red blood cells. Since perfusion
practices vary, it is recommended that each practice verify the use of the CPB
sample type and the length of time in which the CPB sample type should be used
during the recovery period. Note that for hematocrit values above 30 %PCV, the
CPB correction is 1.5 %PCV; the size of the correction at this level should not
impact transfusion decisions.
Lipids Abnormally high lipids may increase results. Interference from lipids will be about
two-thirds the size of the interference from protein.
Rev. Date: 12-Feb-14 Art: 714178-00P Hct - 3
Sodium The sample electrolyte concentration is used to correct the measured conductivity
prior to reporting hematocrit results. Factors that affect sodium will therefore also
affect hematocrit.
Bromide Bromide (37.5 mmol/L) is known to result in an increased rate of star (***) outs.
Bromide has been tested at two levels: the CLSI recommended level and a
therapeutic plasma concentration level of 2.5 mmol/L. The latter is the peak
plasma concentration associated with halothane anesthesia, in which bromide
is released. APOC has not identified a therapeutic condition that would lead to
levels consistent with the CLSI recommended level. Bromide at a concentration of
37.5 mmol/L increased the rate of HCT star (***) outs, while a therapeutic range of
bromide (2.5 mmol/L) did not significantly interfere with i-STAT HCT results.
*It is possible that other interfering substances may be encountered. These results are representative and your results may differ somewhat due to
test-to-test variation. The degree of interference at concentrations other than those listed might not be predictable.
Sample Collection and Handling
Erroneous hematocrit results can be obtained by improper sample handling.
n Hematocrit results can be affected by the settling of red blood cells in the collection device. The
best way to avoid the affect of settling is to test the sample immediately. If there is a delay in
testing of a minute or more, the sample must be remixed thoroughly:
o If the sample is in a collection tube, invert the tube gently 10 times.
o If the sample is in a syringe, roll the syringe between the palms for five seconds in one
direction, then roll in a second direction for five seconds, then gently invert repeatedly for five
seconds. Note that it may not be possible to adequately mix a blood sample in a 1 mL syringe.
Samples from 1 mL syringes should not be used to determine hematocrit if testing is delayed.
Discard one or two drops of blood from a syringe before filling a cartridge.
n Low hematocrit results can be caused by contamination of flush solutions in an arterial or
venous line.
o Back flush a line with a sufficient amount of blood to remove intravenous solutions, heparin or
medications that may contaminate the sample. Five to six times the volume of the catheter,
connectors and needle is recommended.
Cartridge Comparison
The performance characteristics of the sensors are equivalent in all cartridge configurations. System
difference analysis was performed on 40 patient samples using the i-STAT 6+ and i-STAT E3+ cartridges.
In the 1530 %PCV range the average difference was 0.462. In the 3050 %PCV range the average
difference was 0.097.
Calculated Result for Hemoglobin
The i-STAT System provides a calculated hemoglobin result which is determined as follows7:
hemoglobin (g/dL) = hematocrit (% PCV) x 0.34
hemoglobin (g/dL) = hematocrit (decimal fraction) x 34
To convert a hemoglobin result from g/dL to mmol/L, multiply the displayed result by 0.621. The calculation
of hemoglobin from hematocrit assumes a normal MCHC.
Hct - 4 Art: 714178-00P Rev. Date: 12-Feb-14
References
1. D.S. Young, Effects of Drugs on Clinical Laboratory Tests, 3rd ed. (Washington, DC: American
Association of Clinical Chemistry, 1990).
2. CLSI. Procedure for Determining Packed Cell Volume by the Microhematocrit Method; Approved
Standard - Third Edition. CLSI document H7-A3 [ISBN 1-56238-413-9]. CLSI, 940 West Valley Road, Suite
1400, Wayne, Pennsylvania 19087-1898 USA, 2000.
3. B.E. Statland, Clinical Decision Levels for Lab Tests (Oradell, NJ: Medical Economic Books, 1987).
4. CLSI. Method Comparison and Bias Estimation Using Patient Samples; Approved Guideline. CLSI
document EP9-A [ISBN 1-56238-283-7]. CLSI, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania
19087-1898, USA 1995.
5. P.J. Cornbleet and N. Gochman, Incorrect Least-Squares Regression Coefficients in Method-
Comparison Analysis, Clinical Chemistry 25:3, 432 (1979).
6. CLSI. Interference Testing in Clinical Chemistry; Proposed Guideline. CLSI document EP7-P [ISBN 1-
56238-020-6]. CLSI, 940 West Valley Road, Suite 1400, Wayne, Pennsylvania 19087-1898, USA 1986.
7. J.D. Bower, P.G. Ackerman and G. Toto, eds., Evaluation of Formed Elements of Blood, in Clinical
Laboratory Methods (St. Louis: The C.V. Mosby Company, 1974).
i-STAT is a registered trademark of the Abbott Group of Companies in various jurisdictions. Vacutainer is a registered trademark of Becton Dickinson
and Company, Franklin Lakes, NJ USA. Coulter S Plus is a registered trademark of Beckman Coulter Incorporated, Fullerton, CA USA. Cell-Dyn is a
registered trademark of Abbott Laboratories, Abbott Park, IL USA. SE9500 is a trademark of Sysmex America Inc., Mundelein, IL USA. STAT Profile
is a registered trademark of Nova Biomedical, Waltham, MA USA.
Rev. Date: 12-Feb-14 Art: 714178-00P Hct - 5
Abbott Point of Care Inc.
Abbott Park, IL 60064 USA
Emergo Europe
Molenstraat 15
2513 BH, The Hague
The Netherlands
Tel: (31)70 345 8570
Fax: (31)70 346 7299
2014 Abbott Point of Care Inc. All rights reserved. Printed in USA.
Hct - 6 Art: 714178-00P Rev. Date: 12-Feb-14
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Simulated No.1 General Rule:: ExceptDocument29 pagesSimulated No.1 General Rule:: ExceptJie FuentesNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Recalls WordsologyDocument25 pagesRecalls WordsologyJie Fuentes91% (11)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Recall Ascp MirobiologyDocument7 pagesRecall Ascp MirobiologyJie Fuentes80% (5)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Quick Review Cards For Medical Laboratory Science - Polansky, Valerie DietzDocument619 pagesQuick Review Cards For Medical Laboratory Science - Polansky, Valerie DietzIslam92% (86)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Pineapple Upside Down CakeDocument4 pagesPineapple Upside Down CakeJie FuentesNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- F & G Restaurant: SoupsDocument2 pagesF & G Restaurant: SoupsJie FuentesNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Borrower'S Card: Date Borrowe D Item/S Date Returne D Returned byDocument3 pagesBorrower'S Card: Date Borrowe D Item/S Date Returne D Returned byJie FuentesNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Companies Contact Number and QoutationsDocument1 pageCompanies Contact Number and QoutationsJie FuentesNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- En Banc: Imelda Q. Dimaporo, G.R. No. 179285Document11 pagesEn Banc: Imelda Q. Dimaporo, G.R. No. 179285Jie FuentesNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Blood Transfusion Form (NEW)Document1 pageBlood Transfusion Form (NEW)Jie FuentesNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Laboratory Manual and Review On Clinical Pathology PDFDocument32 pagesLaboratory Manual and Review On Clinical Pathology PDFanggaririnNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Nursing Care Plan: Classwork Format Level I CCMC-CN Second Semester A.Y. 2020-2021Document6 pagesNursing Care Plan: Classwork Format Level I CCMC-CN Second Semester A.Y. 2020-2021Mary Ella Mae PilaNo ratings yet
- PolycythemiaDocument3 pagesPolycythemiaSaraNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Avoiding CPSEs - Laboratory Medication Vital SignsDocument30 pagesAvoiding CPSEs - Laboratory Medication Vital SignsForNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- 8 RA 4688 (Clinical Laboratory Law)Document32 pages8 RA 4688 (Clinical Laboratory Law)AIRRA CLAIRE ALVAREZNo ratings yet
- Fluid Mechanics White 7th SOL Part1 Part6Document5 pagesFluid Mechanics White 7th SOL Part1 Part6Jose EscobarNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Blood Tests LabDocument5 pagesBlood Tests LabcoleNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- A Theoretical Model For Blood Flow in Small Vessels: V. P. SrivastavaDocument15 pagesA Theoretical Model For Blood Flow in Small Vessels: V. P. SrivastavaAlinda Fitrotun NisyaNo ratings yet
- CloxacillinDocument8 pagesCloxacillinmcmac24No ratings yet
- Blood Analyses and Anatomy of The Atlantic Salmon: Salmo SalarDocument14 pagesBlood Analyses and Anatomy of The Atlantic Salmon: Salmo SalarSenay MehariNo ratings yet
- Hematocrit AnemiaDocument1 pageHematocrit Anemiadoppler_No ratings yet
- Practical HB HV (Physiology)Document29 pagesPractical HB HV (Physiology)Madonna Hany naeemNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Polycythemia VeraDocument22 pagesPolycythemia VeraMelisande Rae CiruelaNo ratings yet
- Cobas b121 BrochureDocument10 pagesCobas b121 Brochurejuven tusNo ratings yet
- Fluid Electrolyte - Nursing Test QuestionsDocument62 pagesFluid Electrolyte - Nursing Test QuestionsRNStudent1No ratings yet
- Chest Injury QuestionsDocument3 pagesChest Injury QuestionsNicole Genevie MallariNo ratings yet
- Diagnostic and Laboratory TestsDocument85 pagesDiagnostic and Laboratory TestsJamie HaravataNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Table 14 B: Blood Values in The LoridaeDocument7 pagesTable 14 B: Blood Values in The LoridaeahmadNo ratings yet
- Practical Clinical Hematology: Automated Hematology Cell CountersDocument54 pagesPractical Clinical Hematology: Automated Hematology Cell CountersFidaa JaafrahNo ratings yet
- Manual de Usuario - Centrifuga NF 048Document12 pagesManual de Usuario - Centrifuga NF 048Brevas CuchoNo ratings yet
- Shock Case StudyDocument2 pagesShock Case StudyDonna LLerandiNo ratings yet
- Starting A PharmacyDocument8 pagesStarting A PharmacyLloyd Fyl O. RazoNo ratings yet
- Section 13 - Hematology (Updated)Document34 pagesSection 13 - Hematology (Updated)Lorelie CarlosNo ratings yet
- Case Study 1 Nut 116alDocument6 pagesCase Study 1 Nut 116alapi-249635202No ratings yet
- Capillary Puncture Equipment and Procedure PDFDocument23 pagesCapillary Puncture Equipment and Procedure PDFCamille QuiaoitNo ratings yet
- Full Download Book Williams Manual of Hematology 10Th Edition PDFDocument41 pagesFull Download Book Williams Manual of Hematology 10Th Edition PDFronald.jewell170100% (15)
- Understanding CBCDocument9 pagesUnderstanding CBCbettsaltaNo ratings yet
- Hematological Profile of Broilers and Local Chickensin Korhogo, Cote D'IvoireDocument11 pagesHematological Profile of Broilers and Local Chickensin Korhogo, Cote D'IvoireFANKELE ALASSANE KONENo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hematology Laboratory PDFDocument3 pagesHematology Laboratory PDFMariel AbatayoNo ratings yet
- Phlebotomy TestDocument11 pagesPhlebotomy TestRaquel Girón75% (4)