You might also like
- Math Practice Problems Group 3Document2 pagesMath Practice Problems Group 3Lukman Nal 26No ratings yet
- Assessment by Body SystemsDocument2 pagesAssessment by Body SystemsPat McGarryNo ratings yet
- Alcohol DiabetesDocument3 pagesAlcohol DiabeteskoolshotNo ratings yet
- BMC Transitions of CareDocument2 pagesBMC Transitions of Carebalab2311No ratings yet
- What Is Radioactive PollutionDocument4 pagesWhat Is Radioactive PollutionJoy MitraNo ratings yet
- PheochromocytomaDocument2 pagesPheochromocytomaintrovoyz041No ratings yet
- Insulin Types: According To Mode of Action: Rapid Acting Insulin Intermediate Acting Insulin Biphasic InsulinsDocument1 pageInsulin Types: According To Mode of Action: Rapid Acting Insulin Intermediate Acting Insulin Biphasic InsulinsAssem Ashraf Khidhr100% (1)
- Types of Insulin For Diabetes TreatmentDocument8 pagesTypes of Insulin For Diabetes TreatmentChander KantaNo ratings yet
- Cranial NerveDocument4 pagesCranial NerveBrian OballoNo ratings yet
- Assessing Body Temperatur1Document2 pagesAssessing Body Temperatur1juancristoNo ratings yet
- DrUG STUDY PSYCHEDocument52 pagesDrUG STUDY PSYCHELiza MPNo ratings yet
- Aspirn 4Document2 pagesAspirn 4salwaNo ratings yet
- Drug Study: Far Eastern UniversityDocument3 pagesDrug Study: Far Eastern UniversityChoy DacanayNo ratings yet
- Presentation 1Document35 pagesPresentation 1Moitri ChatterjeeNo ratings yet
- Drug Therapy of DM - Oral Antidiabetic DrugsDocument3 pagesDrug Therapy of DM - Oral Antidiabetic DrugsSurria Suguna15No ratings yet
- Anti Diabetik Oral Dan InsulinDocument97 pagesAnti Diabetik Oral Dan InsulinSuci AlimaNo ratings yet
- Diabetes MellitusDocument6 pagesDiabetes Mellitusmaham jahangirNo ratings yet
- Finals PHARMACOTHERAPHY OF DIABETES MELLITUS 2017Document8 pagesFinals PHARMACOTHERAPHY OF DIABETES MELLITUS 2017Sheryl Layne Lao-SebrioNo ratings yet
- Diabetes Drug Chart: Drug Action Use Side Effects Nursing ImplicationsDocument2 pagesDiabetes Drug Chart: Drug Action Use Side Effects Nursing ImplicationspulmonologistNo ratings yet
- Anti Diabetik Oral Dan InsulinDocument97 pagesAnti Diabetik Oral Dan InsulinunknownNo ratings yet
- L12. Endocrine System DrugsDocument12 pagesL12. Endocrine System DrugssabahNo ratings yet
- Drug Name Action Dose & Route Side Effects Nursing Care Brand Name: Twynsta Generic: Telmisartan + AmlodipineDocument4 pagesDrug Name Action Dose & Route Side Effects Nursing Care Brand Name: Twynsta Generic: Telmisartan + AmlodipineEileenAquinoMacapagalNo ratings yet
- Case Clue - 1 LinersDocument753 pagesCase Clue - 1 LinersOnly MrcpNo ratings yet
- Subject: Physiology Topic: Pancreatic Hormones Lecturer: Dr. Gigi Francisco Date: January 2011Document10 pagesSubject: Physiology Topic: Pancreatic Hormones Lecturer: Dr. Gigi Francisco Date: January 2011Std DlshsiNo ratings yet
- Oral Hypoglycemic AgentsDocument38 pagesOral Hypoglycemic Agentsy.gopiNo ratings yet
- Pharmaco - Antidiabetic DrugsDocument2 pagesPharmaco - Antidiabetic DrugsNashrah HusnaNo ratings yet
- Diabetes DrugsDocument1 pageDiabetes Drugsmed testNo ratings yet
- Anti Diabetik Oral Dan InsulinDocument97 pagesAnti Diabetik Oral Dan InsulinLiliaNo ratings yet
- Evogliptin Conference PresentationDocument77 pagesEvogliptin Conference PresentationKrishna Chaitanya100% (1)
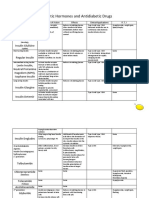
- PHARMA-R4.2-Pancreatic Hormones and Antidiabetic DrugsDocument14 pagesPHARMA-R4.2-Pancreatic Hormones and Antidiabetic Drugscharmainemargaret.parreno.medNo ratings yet
- MetoclopramideDocument1 pageMetoclopramideIvanne Hisoler89% (27)
- Drugs For Diabetes PDFDocument4 pagesDrugs For Diabetes PDFDylan RastoNo ratings yet
- Step 3 - PharmacologyDocument10 pagesStep 3 - PharmacologyLauren LevyNo ratings yet
- 4A Drug SheetDocument14 pages4A Drug SheetTherese PagayNo ratings yet
- Diabetes Treatment: PancreatitisDocument2 pagesDiabetes Treatment: PancreatitisSafiya JamesNo ratings yet
- Drug Name Mechanism of Action Indication Side Effects Nursing Reponsibilities Generic NameDocument4 pagesDrug Name Mechanism of Action Indication Side Effects Nursing Reponsibilities Generic NamehahahaNo ratings yet
- Linagliptin - DRUG STUDYDocument1 pageLinagliptin - DRUG STUDYAcads useNo ratings yet
- The Endocrine Pancreas & The Control of Blood Glucose: 1. A-Cells (20%)Document63 pagesThe Endocrine Pancreas & The Control of Blood Glucose: 1. A-Cells (20%)Ledia EssamNo ratings yet
- Therapeutics Diabetes DrugchartDocument4 pagesTherapeutics Diabetes DrugchartSharan SahotaNo ratings yet
- Drugstudy Case StudyDocument7 pagesDrugstudy Case StudyHerwincayeNo ratings yet
- Drug Study 2Document5 pagesDrug Study 2Bani Ann Dela CruzNo ratings yet
- Name of Drug Mechanism of Action Indications Contraindication Side Effects Nursing Responsibilities Generic Name: BeforeDocument5 pagesName of Drug Mechanism of Action Indications Contraindication Side Effects Nursing Responsibilities Generic Name: BeforeWestley RubinoNo ratings yet
- DM PDFDocument35 pagesDM PDFMuhammad Sofwan agungNo ratings yet
- Drug StudyDocument5 pagesDrug StudyJanika BecieraNo ratings yet
- Physiology DiabetesDocument48 pagesPhysiology Diabetesrajesh g100% (1)
- Generic NameDocument5 pagesGeneric NameJanika BecieraNo ratings yet
- By Dr. Marita FuentesDocument5 pagesBy Dr. Marita Fuentes2013SecBNo ratings yet
- Drug Study IsoniazidDocument3 pagesDrug Study IsoniazidJamil Lorca100% (4)
- Insulin and Antidiabetic Drugs: BSC Nursing Online and Offline Lecture SeriesDocument27 pagesInsulin and Antidiabetic Drugs: BSC Nursing Online and Offline Lecture SeriesSayan ChatterjeeNo ratings yet
- Pancreatic Hormones and Antidiabetic DrugsDocument6 pagesPancreatic Hormones and Antidiabetic DrugsCas BuNo ratings yet
- Pathophysiology of Diabetes MellitusDocument62 pagesPathophysiology of Diabetes MellitusNicee SelpaNo ratings yet
- Drugs For DiabetesDocument8 pagesDrugs For DiabetesUsmanNo ratings yet
- StudyDocument5 pagesStudyWestley RubinoNo ratings yet
- Simplify Insulin Therapy With IDegAsp Co-Formulation - 2022 UpdtDocument21 pagesSimplify Insulin Therapy With IDegAsp Co-Formulation - 2022 UpdtTataNo ratings yet
- IT 10 - Farmakologi Obat - Obat Di Bidang Endokrin - TEODocument34 pagesIT 10 - Farmakologi Obat - Obat Di Bidang Endokrin - TEOtattosssNo ratings yet
- Drug Index Patient 2203Document3 pagesDrug Index Patient 2203Arienne_Mae_A__6554No ratings yet
- Shock Acute Myocardial Infarction Septicemia Precautions Diabetic KetoacidosisDocument3 pagesShock Acute Myocardial Infarction Septicemia Precautions Diabetic KetoacidosisArienne_Mae_A__6554No ratings yet
- Table 1. Antihyperglycemic Agents For Use in Type 2 DiabetesDocument5 pagesTable 1. Antihyperglycemic Agents For Use in Type 2 DiabeteszeiarraNo ratings yet
- Pharmacology - Section 25 - Insulin and HypoglycaemicsDocument3 pagesPharmacology - Section 25 - Insulin and HypoglycaemicsPathalee ThalpavilaNo ratings yet
- Insulin Resistance: Divisi Endokrin-Metabolik Departemen Ilmu Penyakit Dalam FK USU / RSUP HAM MedanDocument36 pagesInsulin Resistance: Divisi Endokrin-Metabolik Departemen Ilmu Penyakit Dalam FK USU / RSUP HAM MedanPaul Behring ManurungNo ratings yet
- Urinary Concentration and DilutionDocument10 pagesUrinary Concentration and DilutionAbhineeth BhatNo ratings yet
- Guide To BoardsDocument3 pagesGuide To BoardsAbhineeth BhatNo ratings yet
- STEP1 ResourcesDocument2 pagesSTEP1 ResourcesAbhineeth BhatNo ratings yet
- Approved: HFHS Nov-June Only HFH Has No PrerequisitesDocument1 pageApproved: HFHS Nov-June Only HFH Has No PrerequisitesAbhineeth BhatNo ratings yet
- Question PhilosophyDocument3 pagesQuestion PhilosophyAbhineeth BhatNo ratings yet
- Aging and MenopauseDocument3 pagesAging and MenopauseAbhineeth BhatNo ratings yet
- Pathophys - Endocrine - LipoproteinsDocument4 pagesPathophys - Endocrine - LipoproteinsAbhineeth BhatNo ratings yet
- Gi HyDocument2 pagesGi HyAbhineeth BhatNo ratings yet
- Daftar ObatDocument9 pagesDaftar ObatMuhammad Rizki ImannudinNo ratings yet
- 2018-July MIMS DoctorDocument44 pages2018-July MIMS Doctoryulia dwiNo ratings yet
- GNM Vol IV Nursing Foundation Part 3 MinDocument462 pagesGNM Vol IV Nursing Foundation Part 3 MinJasmine PraveenNo ratings yet
- Sodium Polystyrene SulfonateDocument11 pagesSodium Polystyrene SulfonatejanellaNo ratings yet
- Medicine Comprehension WorksheetDocument3 pagesMedicine Comprehension WorksheetAna Angeleska-SpiroskaNo ratings yet
- MBBS Antiarrhythmics 2014 Class II (Antiarrhythmic Drugs)Document23 pagesMBBS Antiarrhythmics 2014 Class II (Antiarrhythmic Drugs)Dr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Pharmacology-I II Pharm.D. Question BankDocument6 pagesPharmacology-I II Pharm.D. Question BankAnanda Vijayasarathy100% (1)
- Ati PharmacologyDocument24 pagesAti PharmacologySarah Rice95% (38)
- Harga Catalog PT - Igm 2020Document4 pagesHarga Catalog PT - Igm 2020yandiNo ratings yet
- Formulation Development and Evaluation of Buccal Tablets of PantoprazoleDocument6 pagesFormulation Development and Evaluation of Buccal Tablets of PantoprazoleBaru Chandrasekhar RaoNo ratings yet
- Interaction Part 1Document10 pagesInteraction Part 1PRINCE AHAD MIRNo ratings yet
- CA DIAGNOSTIC TEST Copy 1Document11 pagesCA DIAGNOSTIC TEST Copy 1Ermita AaronNo ratings yet
- Gout Paijit PDFDocument46 pagesGout Paijit PDFKiattipoom SukkulcharoenNo ratings yet
- From Idea To MarketDocument6 pagesFrom Idea To MarketvictorccNo ratings yet
- CTD Ectd Ra KDocument24 pagesCTD Ectd Ra KGautami UbhraniNo ratings yet
- Drug Study SittieDocument8 pagesDrug Study SittieHarrisha G SanduyoganNo ratings yet
- Glipizide Has The Shortest Half-Life (2-4 Hours) of The More Potent Agents. ForDocument2 pagesGlipizide Has The Shortest Half-Life (2-4 Hours) of The More Potent Agents. ForR Eka PutraNo ratings yet
- Penulisan Resep Yang Baik Dan BenarDocument2 pagesPenulisan Resep Yang Baik Dan BenarEdward KurniawanNo ratings yet
- Diabetes Medications Chart PDFDocument1 pageDiabetes Medications Chart PDFRachel Lalaine Marie SialanaNo ratings yet
- Clomipramine PDFDocument18 pagesClomipramine PDFddandan_2No ratings yet
- 1.1 Intro To BiopharmDocument32 pages1.1 Intro To BiopharmNeha Dand100% (1)
- Final EthicsDocument19 pagesFinal EthicsSheel Gautam100% (1)
- 1745-Article Text-6947-2-10-20200624Document14 pages1745-Article Text-6947-2-10-20200624Gaurav AdhikariNo ratings yet
- Cal Misbah Test 2016 Qa PDFDocument51 pagesCal Misbah Test 2016 Qa PDFSyedKashifAliNo ratings yet
- Ranitidine NeomedDocument5 pagesRanitidine NeomedMarsyaNo ratings yet
- Xylazine-Involved Overdose Deaths FINAL - 3.8.23Document5 pagesXylazine-Involved Overdose Deaths FINAL - 3.8.23ActionNewsJaxNo ratings yet
- Pharmacology Related To Psychiatric Nursing PDFDocument14 pagesPharmacology Related To Psychiatric Nursing PDFAnonymous nEQNlgbYQCNo ratings yet
- Responsi KapsulDocument3 pagesResponsi KapsulGeby FransiscaNo ratings yet
- Daftar Obat High Alert MedicationDocument7 pagesDaftar Obat High Alert Medicationlala bestgirlNo ratings yet
- Abq Pharmaceutics Nidhi MishraDocument11 pagesAbq Pharmaceutics Nidhi MishranidhiNo ratings yet