You might also like
- Basic Objectives of Color and Spectral DopplerDocument5 pagesBasic Objectives of Color and Spectral DopplerAsaad Baloch100% (2)
- Redo CabgDocument36 pagesRedo CabgSantanico De CVT deozaNo ratings yet
- Stroke Cerebrovascular Disease CVA Cerebral Infarction Cerebral Hemorrhage Ischemic Stroke Stroke - IschemicDocument47 pagesStroke Cerebrovascular Disease CVA Cerebral Infarction Cerebral Hemorrhage Ischemic Stroke Stroke - Ischemickarina lestariNo ratings yet
- Aortic StenosisDocument35 pagesAortic StenosisMuhd SyazwanNo ratings yet
- Carotid Artery DiseaseDocument48 pagesCarotid Artery DiseaseAdeleye John AdebolaNo ratings yet
- SURG 4.04 Thoracic Aortic Aneurysm - Aortic Dissection - Dr. Achurra (Updated + Additional Pics)Document8 pagesSURG 4.04 Thoracic Aortic Aneurysm - Aortic Dissection - Dr. Achurra (Updated + Additional Pics)Monique BorresNo ratings yet
- IntroductionDocument8 pagesIntroductionwan hanisaNo ratings yet
- #0、aneurysmDocument39 pages#0、aneurysmMargaret ThatcherNo ratings yet
- Caso Clinico 3 CompressedDocument20 pagesCaso Clinico 3 Compressedapi-703195004No ratings yet
- Cardiac Conduction System Power Point PresentationDocument30 pagesCardiac Conduction System Power Point PresentationAaya AdelNo ratings yet
- IrcerebralDocument30 pagesIrcerebralJamel MacasNo ratings yet
- Procedures On Thoracic Aorta: Sean P Roddy, MDDocument16 pagesProcedures On Thoracic Aorta: Sean P Roddy, MDUmer AhmadNo ratings yet
- TIADocument22 pagesTIAArabylle Maranca AbuelNo ratings yet
- Northwestern Medicine Percutaneous Coronary Intervention Pci NMHDocument8 pagesNorthwestern Medicine Percutaneous Coronary Intervention Pci NMHRamses DagoyNo ratings yet
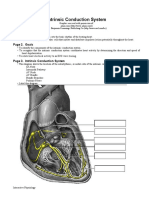
- Intrinsic Conduction System: Page 1. IntroductionDocument5 pagesIntrinsic Conduction System: Page 1. IntroductionUta Provinsiana SukmaraNo ratings yet
- Surgical Recall Vascular SurgeryDocument28 pagesSurgical Recall Vascular SurgeryAltariaNo ratings yet
- Cardiac Catheterization: Pacemaker, Rfa, Nerve Block: Sehrish ManzoorDocument32 pagesCardiac Catheterization: Pacemaker, Rfa, Nerve Block: Sehrish ManzoorZainNo ratings yet
- Intracardiac Echo DR SrikanthDocument107 pagesIntracardiac Echo DR SrikanthNakka SrikanthNo ratings yet
- Cardiac Pacing For The SurgeonsDocument46 pagesCardiac Pacing For The SurgeonsRezwanul Hoque BulbulNo ratings yet
- Indications: PurposeDocument13 pagesIndications: PurposeIRA ODETTE GATUSNo ratings yet
- Biofluid Assignment 3Document6 pagesBiofluid Assignment 3Dina AssefaNo ratings yet
- An Approach To ECGDocument42 pagesAn Approach To ECGGIST (Gujarat Institute of Science & Technology)No ratings yet
- Catheter Ablation For AFDocument12 pagesCatheter Ablation For AFPeny Ruth Jessica DamanikNo ratings yet
- The Echo Exam: Echo Findings in EndocarditisDocument1 pageThe Echo Exam: Echo Findings in EndocarditisYanNo ratings yet
- FghjiuytDocument1 pageFghjiuytYanNo ratings yet
- CompressedDocument73 pagesCompressedapi-667225436No ratings yet
- Unit 6 Cardiac Catheterization and AngiographyDocument28 pagesUnit 6 Cardiac Catheterization and AngiographyJack Tomar100% (1)
- Anato IMAO BrainDocument220 pagesAnato IMAO BrainVilasecaNo ratings yet
- Pastest Note 1Document3 pagesPastest Note 1Amer AldhaliaNo ratings yet
- Fundamentals of ECGDocument112 pagesFundamentals of ECGadithya polavarapu100% (1)
- Radiologi KardiovaskularDocument59 pagesRadiologi KardiovaskularNhaNa HikmAtulNo ratings yet
- Us Abdominal AortaDocument16 pagesUs Abdominal AortaRomaNo ratings yet
- Jead 024Document21 pagesJead 024wassim wassimNo ratings yet
- Aneurysms & Aortic DissectionDocument36 pagesAneurysms & Aortic Dissectionr100% (1)
- Case Report MMMMa Atul & RajDocument36 pagesCase Report MMMMa Atul & RajalkaNo ratings yet
- Neuro Module Part 1Document194 pagesNeuro Module Part 1Gabriel GhiațăNo ratings yet
- EcgDocument34 pagesEcgSundara Rami ReddyNo ratings yet
- Invasive Cardiology LectureDocument49 pagesInvasive Cardiology LectureJibran Jones GarciaNo ratings yet
- Neurology NotesDocument15 pagesNeurology NotesAshley Diane Henry100% (3)
- Lab 2 - The HeartDocument5 pagesLab 2 - The HeartTaydonNo ratings yet
- NUR3111 Post-Lecture QuizDocument28 pagesNUR3111 Post-Lecture QuizliNo ratings yet
- EcgDocument11 pagesEcgRajneesh TiwariNo ratings yet
- Arterial Supply of Head and NeckDocument41 pagesArterial Supply of Head and NeckKhadija VasiNo ratings yet
- (PDF.3) Management of Heart AttackDocument33 pages(PDF.3) Management of Heart AttackTheany Be SmilerNo ratings yet
- Overview of NeuroangiographyDocument9 pagesOverview of Neuroangiographynaren_winv1350No ratings yet
- Gibson 2013Document14 pagesGibson 2013Moisés Alberto CharajaNo ratings yet
- Percutaneous Coronary Intervention 10 05Document8 pagesPercutaneous Coronary Intervention 10 05benypermadiNo ratings yet
- EKG ATLAS InterpretationDocument316 pagesEKG ATLAS InterpretationDumitrescu Roxana100% (1)
- TEE For ImpellaDocument6 pagesTEE For ImpellaPriya Nair MenonNo ratings yet
- Cardiac CatheterizationDocument6 pagesCardiac CatheterizationUzma KhanNo ratings yet
- Isolated Right Ventricular Myocardial Infarction: A Case ReportDocument5 pagesIsolated Right Ventricular Myocardial Infarction: A Case ReportNadyaindriati96No ratings yet
- Ultrasound Procedures1Document9 pagesUltrasound Procedures1ramilccabrigaNo ratings yet
- Anatomy Formative Preview of Thorax and BackDocument22 pagesAnatomy Formative Preview of Thorax and Backmvs hardhikNo ratings yet
- Aortic DissectionDocument14 pagesAortic Dissectionapi-3733922100% (2)
- PacemakersDocument38 pagesPacemakersrebebravoiniguez642No ratings yet
- Valvular Surgerys and ProsthesisDocument7 pagesValvular Surgerys and ProsthesisArunNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- James Chen - Head and Neck Imaging PDFDocument83 pagesJames Chen - Head and Neck Imaging PDFdamclf100% (1)
- Askep Ps DGN Tindakan Invasif & INB KD 2021Document91 pagesAskep Ps DGN Tindakan Invasif & INB KD 2021gayuspatarru123No ratings yet
- Decoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonFrom EverandDecoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonAfzal SohaibNo ratings yet
- Radiographic Pathology ReviewerDocument479 pagesRadiographic Pathology ReviewerMark M. AlipioNo ratings yet
- Food DeliveryDocument3 pagesFood DeliveryMark M. AlipioNo ratings yet
- SkullDocument19 pagesSkullMark M. Alipio100% (1)
- Radiation Therapy: Khan BentelDocument9 pagesRadiation Therapy: Khan BentelMark M. AlipioNo ratings yet
- Philosophy Statement " Aestimamus Vitam "Document4 pagesPhilosophy Statement " Aestimamus Vitam "Mark M. AlipioNo ratings yet
- Research TopicsDocument1 pageResearch TopicsMark M. AlipioNo ratings yet
- Anaphysio ProfpquizDocument9 pagesAnaphysio ProfpquizMark M. AlipioNo ratings yet
- Radiation Therapy: Khan BentelDocument9 pagesRadiation Therapy: Khan BentelMark M. AlipioNo ratings yet
- Review RadiotechDocument587 pagesReview RadiotechMark M. AlipioNo ratings yet
- Radiation Biology and PhysicsDocument4 pagesRadiation Biology and PhysicsMark M. AlipioNo ratings yet
- ReferencesDocument2 pagesReferencesMark M. AlipioNo ratings yet
- Nmat Answer Key-PhysicsDocument5 pagesNmat Answer Key-PhysicsNina Charlyn AlbaNo ratings yet
- Radiographic TestingDocument47 pagesRadiographic TestingsmrndrdasNo ratings yet
- 01 - Basic Physics 2011 PDFDocument13 pages01 - Basic Physics 2011 PDFMark M. AlipioNo ratings yet
- Sustainability 09 01823Document16 pagesSustainability 09 01823Mark M. AlipioNo ratings yet
- Final ThesisDocument147 pagesFinal ThesisMark M. AlipioNo ratings yet
- Goals: Principles of Imaging Science IDocument13 pagesGoals: Principles of Imaging Science INeeraj JangidNo ratings yet
- Radiation Physics LectureDocument272 pagesRadiation Physics LectureMark M. AlipioNo ratings yet
- Air Embolism Diagnosed by Doppler Ultrasound .25Document4 pagesAir Embolism Diagnosed by Doppler Ultrasound .25Mark M. AlipioNo ratings yet
- Supp Hip OnlyDocument20 pagesSupp Hip OnlyMark M. AlipioNo ratings yet
- NCLEX Test ReviewDocument7 pagesNCLEX Test ReviewPhuong Tran100% (1)
- Blaivas 2004Document5 pagesBlaivas 2004Mark M. AlipioNo ratings yet
- Acing The Orthopedic Board ExamDocument481 pagesAcing The Orthopedic Board ExamMark M. Alipio100% (9)
- Practice Quiz Answers Unit 1Document5 pagesPractice Quiz Answers Unit 1Marvin BautistaNo ratings yet
- Amundson Basic Biology PDFDocument13 pagesAmundson Basic Biology PDFFernanda RibeiroNo ratings yet
- Print Foundations - Fundamentals of Nursing, Chapter 48 Skin Integrity and Wound Care Flashcards - Easy NotecardsDocument6 pagesPrint Foundations - Fundamentals of Nursing, Chapter 48 Skin Integrity and Wound Care Flashcards - Easy NotecardsMark M. AlipioNo ratings yet
- Survey Radiobiology 2012Document11 pagesSurvey Radiobiology 2012Mark M. AlipioNo ratings yet
- 2014528175541Document20 pages2014528175541Mark M. AlipioNo ratings yet
- 203 AbDocument39 pages203 AbMark M. AlipioNo ratings yet
- APP05Document3 pagesAPP05Roberto Giorgio N. PachecoNo ratings yet
- High School Bukit MertajamDocument25 pagesHigh School Bukit MertajamrisliNo ratings yet
- Drug Study AtorvastatinDocument1 pageDrug Study AtorvastatinEzron Kendrick DuranNo ratings yet
- Group 1 - Final PracticumDocument6 pagesGroup 1 - Final PracticumRiz Ann ZaragozaNo ratings yet
- Live Well, Live LongDocument432 pagesLive Well, Live Longpartis5555No ratings yet
- NCM 106 Acute Biologic CrisisDocument142 pagesNCM 106 Acute Biologic CrisisEllamae Chua88% (8)
- Homeopathy For Chronic Renal FailureDocument15 pagesHomeopathy For Chronic Renal FailureProfRajakumar Dvr100% (1)
- Human Diseases A Systemic Approach 8th Edition-Páginas-15-26Document12 pagesHuman Diseases A Systemic Approach 8th Edition-Páginas-15-26Karime LopezNo ratings yet
- SmokingDocument27 pagesSmokingOwe SagumNo ratings yet
- Report Go Kart CatiaDocument29 pagesReport Go Kart CatiaFaiz HaikalNo ratings yet
- Nuclear Cardiology Study Guide: Andrzej Moniuszko B. Adrian KesalaDocument293 pagesNuclear Cardiology Study Guide: Andrzej Moniuszko B. Adrian KesalaAnuNo ratings yet
- What Is Alcohol2012AAlisherMDPhDDocument58 pagesWhat Is Alcohol2012AAlisherMDPhDAlisher AgzamovNo ratings yet
- Extra Yds Deneme Sinavi 9Document20 pagesExtra Yds Deneme Sinavi 9atalikaci100% (1)
- Heart Disease: Prevention Is Better Than CureDocument3 pagesHeart Disease: Prevention Is Better Than CureTan Soong WeiNo ratings yet
- MNG - D1 - 4. Rehabilitation Guideline of Myocardial Infarction PDFDocument83 pagesMNG - D1 - 4. Rehabilitation Guideline of Myocardial Infarction PDFRaagulan JeyashankerNo ratings yet
- MEDS90001 Population Health Assignment 2012Document3 pagesMEDS90001 Population Health Assignment 2012Margaret AyersNo ratings yet
- CHD With NCPDocument10 pagesCHD With NCPJohanna Kirsten F. DaguioNo ratings yet
- Hypertension PDFDocument7 pagesHypertension PDFAnonymous irviEcaraNo ratings yet
- Rujuk FebDocument171 pagesRujuk FebGemma AyuNo ratings yet
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919No ratings yet
- (CLINPHAR) 2015 Clinical Practice Guidelines For The Management of Dyslipidemia in The Philippines - ExtractedDocument44 pages(CLINPHAR) 2015 Clinical Practice Guidelines For The Management of Dyslipidemia in The Philippines - ExtractedDenise Yanci DemiarNo ratings yet
- Ischemic Cardiac DiseaseDocument34 pagesIschemic Cardiac DiseaseGopala HariNo ratings yet
- Screenshot 2023-02-26 at 4.12.17 PM PDFDocument80 pagesScreenshot 2023-02-26 at 4.12.17 PM PDFAsyari HaxenNo ratings yet
- NURSING CARE PLAN For Myocardial InfarctionDocument16 pagesNURSING CARE PLAN For Myocardial InfarctionFreisanChenMandumotan100% (1)
- Lipid Transport and StorageDocument34 pagesLipid Transport and StorageGuru Kiran C KNo ratings yet
- Lyon Diet Heart StudyDocument7 pagesLyon Diet Heart StudyElaine June FielNo ratings yet
- Yr10 Heart LDocument8 pagesYr10 Heart Lspamzz063No ratings yet
- Cardiovascular System: AnatomyDocument19 pagesCardiovascular System: AnatomyStephanie MacVeighNo ratings yet
- Unit 1 Concepts of Physical FitnessDocument116 pagesUnit 1 Concepts of Physical FitnessnanaNo ratings yet
- Clinical Trials in Cardiology 2nd Ed PDFDocument272 pagesClinical Trials in Cardiology 2nd Ed PDFIrving H Torres LopezNo ratings yet
- PaytmDocument44 pagesPaytmBirendra ChaudharyNo ratings yet