You might also like
- Isthmus Flap Aortoplasty For Repair of Long Segment Coarctation AortaDocument10 pagesIsthmus Flap Aortoplasty For Repair of Long Segment Coarctation AortaJose YoveraNo ratings yet
- Surgical Outcomes of DVAPTRepairDocument11 pagesSurgical Outcomes of DVAPTRepairJose YoveraNo ratings yet
- Bidirectional Cavopulmonary Shunt With Additional PBF - Gerelli2012Document7 pagesBidirectional Cavopulmonary Shunt With Additional PBF - Gerelli2012Jose YoveraNo ratings yet
- Warden 1984Document5 pagesWarden 1984Jose YoveraNo ratings yet
- Surgical Treatment of Partial Anomalous Pulmonary Venous Connection To The Superior Vena CavaDocument5 pagesSurgical Treatment of Partial Anomalous Pulmonary Venous Connection To The Superior Vena CavaJose YoveraNo ratings yet
- Chandra 2013Document5 pagesChandra 2013Jose YoveraNo ratings yet
- Vargas 1985Document4 pagesVargas 1985Jose YoveraNo ratings yet
- 2013 Cardiac Pacing and CRT 2013 ESC GuidelineDocument49 pages2013 Cardiac Pacing and CRT 2013 ESC GuidelineTony Gomez Luna LeyvaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ashp - Midyear PosterDocument1 pageAshp - Midyear Posterapi-611918048No ratings yet
- (The European Society of Cardiology Series) Marco Tubaro (Editor), Pascal Vranckx (Editor), Susanna Price (Editor), Christiaan Vrints (Editor), Eric Bonnefoy (Editor) - The ESC Textbook of Intensive ADocument1,088 pages(The European Society of Cardiology Series) Marco Tubaro (Editor), Pascal Vranckx (Editor), Susanna Price (Editor), Christiaan Vrints (Editor), Eric Bonnefoy (Editor) - The ESC Textbook of Intensive AEdu MartinsNo ratings yet
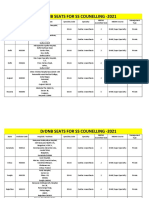
- Final DRDNB Seats For SS Counselling 2021Document152 pagesFinal DRDNB Seats For SS Counselling 2021Pavan KumarNo ratings yet
- ACLS and MegacodeDocument33 pagesACLS and MegacodeMark Joseph100% (1)
- Soal MAYO Yg KeluarDocument8 pagesSoal MAYO Yg KeluardoktersaktiNo ratings yet
- Aortic RegurgitationDocument2 pagesAortic RegurgitationMalueth AnguiNo ratings yet
- Cardiac Stent PriceDocument4 pagesCardiac Stent PriceMahmudul Hasan TusharNo ratings yet
- Aha 2014Document123 pagesAha 2014Nereida AceitunoNo ratings yet
- Cardiac Rhythms - ECG ReadingsDocument15 pagesCardiac Rhythms - ECG Readingsal-obinay shereenNo ratings yet
- Cardiovascular SystemDocument8 pagesCardiovascular SystemDawnmurph Dharlene Wag-eNo ratings yet
- Cardiogenic ShockDocument31 pagesCardiogenic ShockWisnu WardhanaNo ratings yet
- Iccu / Cicu: Patients Heart Attacks Unstable Angina Cardiac DysrhythmiaDocument4 pagesIccu / Cicu: Patients Heart Attacks Unstable Angina Cardiac DysrhythmiaAlya Putri KhairaniNo ratings yet
- Dayanand Medical College and Hospital Ludhiana BrochureDocument71 pagesDayanand Medical College and Hospital Ludhiana BrochureManoj KumarNo ratings yet
- Chapter 1Document2 pagesChapter 1longaitiNo ratings yet
- ESMRDocument23 pagesESMRbiogene_bdNo ratings yet
- Topnotch ECG Interpretation For MoonlightersDocument25 pagesTopnotch ECG Interpretation For Moonlightersmefav7778520100% (1)
- Advanced Heart Failure: A Position Statementof The Heart Failure Association of Theeuropean Society of CardiologyDocument11 pagesAdvanced Heart Failure: A Position Statementof The Heart Failure Association of Theeuropean Society of CardiologyFlorentino Remon GodoyNo ratings yet
- Presented by DR Rahul D AgrawalDocument64 pagesPresented by DR Rahul D AgrawalRahul AgrawalNo ratings yet
- Hilarie Rankin CVDocument2 pagesHilarie Rankin CVapi-555062409No ratings yet
- Electrocardiogram: By: Keverne Jhay P. Colas, RN, MANDocument72 pagesElectrocardiogram: By: Keverne Jhay P. Colas, RN, MANGaras AnnaBerniceNo ratings yet
- Anti Anginal DrugsDocument26 pagesAnti Anginal DrugsAtharva PuranikNo ratings yet
- Simulation Acute Coronary Syndrome (Learner)Document2 pagesSimulation Acute Coronary Syndrome (Learner)Wanda Nowell0% (1)
- Prosthetic Heart ValvesDocument50 pagesProsthetic Heart ValvesArtemisNo ratings yet
- Pharmacology AnginaDocument28 pagesPharmacology AnginaalijanmarwatNo ratings yet
- Discharge Planning PaperDocument5 pagesDischarge Planning Paperapi-398485408No ratings yet
- 150 Ecg Cases Fifth Edition John Hampton Full Chapter PDF ScribdDocument67 pages150 Ecg Cases Fifth Edition John Hampton Full Chapter PDF Scribdbrandon.jackson228100% (5)
- Electrocardiogram EcgDocument10 pagesElectrocardiogram EcgBaha'aeddin HammadNo ratings yet
- Ischemic Heart DiseaseDocument116 pagesIschemic Heart DiseaseAndrew OrlovNo ratings yet
- Some PDFDocument55 pagesSome PDFFred SmytheNo ratings yet
- Heart Failure Clinical Presentation - History, Physical Examination, Predominant Right-Sided Heart FailureDocument9 pagesHeart Failure Clinical Presentation - History, Physical Examination, Predominant Right-Sided Heart FailureAizel ManiagoNo ratings yet