You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Pengaruh Hiperglemi Terhadap Peran Sitoskeleton Cytoskeleton (DR RudijantoDocument15 pagesPengaruh Hiperglemi Terhadap Peran Sitoskeleton Cytoskeleton (DR RudijantoAliyah SajaNo ratings yet
- Atopic Dermatitis 2013Document45 pagesAtopic Dermatitis 2013Christopher ShawNo ratings yet
- Jurnal MorbiliDocument5 pagesJurnal MorbiliAlbert ChristianNo ratings yet
- Jurnal MorbiliDocument8 pagesJurnal MorbiliNely KeybumNo ratings yet
- Treatment of Otitis Media With Effusion Based On Politzerization With An Automated DeviceDocument5 pagesTreatment of Otitis Media With Effusion Based On Politzerization With An Automated DeviceChristopher ShawNo ratings yet
- PDFDocument32 pagesPDFChristopher ShawNo ratings yet
- PDFDocument32 pagesPDFChristopher ShawNo ratings yet
- Health sector responses to sexual violence and its victimsDocument133 pagesHealth sector responses to sexual violence and its victimssssildiko4763No ratings yet
- Treatment of Otitis Media With Effusion Based On Politzerization With An Automated DeviceDocument5 pagesTreatment of Otitis Media With Effusion Based On Politzerization With An Automated DeviceChristopher ShawNo ratings yet
- New Therapeutic Strategy For Treating Otitis Media With Effusion in Postirradiated Nasopharyngeal Carcinoma PatientsDocument6 pagesNew Therapeutic Strategy For Treating Otitis Media With Effusion in Postirradiated Nasopharyngeal Carcinoma PatientsChristopher ShawNo ratings yet
- Treatment of Otitis Media With Effusion Based On Politzerization With An Automated DeviceDocument5 pagesTreatment of Otitis Media With Effusion Based On Politzerization With An Automated DeviceChristopher ShawNo ratings yet
- Gynecologic EmergenciesDocument21 pagesGynecologic EmergenciesChristopher ShawNo ratings yet
- OME (Glue Ear) / Adenoid and Grommet: Position Paper ENT UK 2009Document4 pagesOME (Glue Ear) / Adenoid and Grommet: Position Paper ENT UK 2009Christopher ShawNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- MSBI Installation GuideDocument25 pagesMSBI Installation GuideAmit SharmaNo ratings yet
- 4Q Labor Case DigestsDocument53 pages4Q Labor Case DigestsKaren Pascal100% (2)
- Las Q1Document9 pagesLas Q1Gaux SkjsjaNo ratings yet
- Deed of Sale - Motor VehicleDocument4 pagesDeed of Sale - Motor Vehiclekyle domingoNo ratings yet
- Enerflex 381338Document2 pagesEnerflex 381338midoel.ziatyNo ratings yet
- Chapter 6: Structured Query Language (SQL) : Customer Custid Custname OccupationDocument16 pagesChapter 6: Structured Query Language (SQL) : Customer Custid Custname OccupationSarmila MahendranNo ratings yet
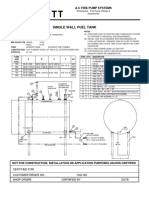
- Single Wall Fuel Tank: FP 2.7 A-C Fire Pump SystemsDocument1 pageSingle Wall Fuel Tank: FP 2.7 A-C Fire Pump Systemsricardo cardosoNo ratings yet
- C79 Service Kit and Parts List GuideDocument32 pagesC79 Service Kit and Parts List Guiderobert100% (2)
- Royal Enfield Market PositioningDocument7 pagesRoyal Enfield Market PositioningApoorv Agrawal67% (3)
- Excavator Loading To Truck TrailerDocument12 pagesExcavator Loading To Truck TrailerThy RonNo ratings yet
- SyllabusDocument4 pagesSyllabusapi-105955784No ratings yet
- Venturi Meter and Orifice Meter Flow Rate CalculationsDocument2 pagesVenturi Meter and Orifice Meter Flow Rate CalculationsVoora GowthamNo ratings yet
- 04 Dasmarinas Vs Reyes GR No 108229Document2 pages04 Dasmarinas Vs Reyes GR No 108229Victoria Melissa Cortejos PulidoNo ratings yet
- Gps Anti Jammer Gpsdome - Effective Protection Against JammingDocument2 pagesGps Anti Jammer Gpsdome - Effective Protection Against JammingCarlos VillegasNo ratings yet
- FEM Lecture Notes-2Document18 pagesFEM Lecture Notes-2macynthia26No ratings yet
- Milwaukee 4203 838a PB CatalogaciónDocument2 pagesMilwaukee 4203 838a PB CatalogaciónJuan carlosNo ratings yet
- Well Control Kill Sheet (Low Angle Wells)Document8 pagesWell Control Kill Sheet (Low Angle Wells)Tatita ValenciaNo ratings yet
- BAR Digest MenuDocument4 pagesBAR Digest MenuFloila Jane YmasNo ratings yet
- LPM 52 Compar Ref GuideDocument54 pagesLPM 52 Compar Ref GuideJimmy GilcesNo ratings yet
- MN AG v. SANOFI - 3:18-cv-14999 - Defendants' Joint Motion To Dismiss - 2019-08-12Document124 pagesMN AG v. SANOFI - 3:18-cv-14999 - Defendants' Joint Motion To Dismiss - 2019-08-12The Type 1 Diabetes Defense FoundationNo ratings yet
- NAC Case Study AnalysisDocument25 pagesNAC Case Study AnalysisSushma chhetriNo ratings yet
- CompactLogix 5480 Controller Sales GuideDocument2 pagesCompactLogix 5480 Controller Sales GuideMora ArthaNo ratings yet
- Eritrea and Ethiopia Beyond The Impasse PDFDocument12 pagesEritrea and Ethiopia Beyond The Impasse PDFThe Ethiopian AffairNo ratings yet
- 2.8 V6 5V (Aha & Atq)Document200 pages2.8 V6 5V (Aha & Atq)Vladimir Socin ShakhbazyanNo ratings yet
- Backup and Recovery ScenariosDocument8 pagesBackup and Recovery ScenariosAmit JhaNo ratings yet
- ABBBADocument151 pagesABBBAJeremy MaraveNo ratings yet
- Learning HotMetal Pro 6 - 132Document332 pagesLearning HotMetal Pro 6 - 132Viên Tâm LangNo ratings yet
- (Free Scores - Com) - Stumpf Werner Drive Blues en Mi Pour La Guitare 40562 PDFDocument2 pages(Free Scores - Com) - Stumpf Werner Drive Blues en Mi Pour La Guitare 40562 PDFAntonio FresiNo ratings yet
- SAP PS Step by Step OverviewDocument11 pagesSAP PS Step by Step Overviewanand.kumarNo ratings yet
- Terms and Condition PDFDocument2 pagesTerms and Condition PDFSeanmarie CabralesNo ratings yet