You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Data and Analytics Framework v2 PDFDocument2 pagesData and Analytics Framework v2 PDFquangthang92No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- New Microsoft Word DocumentDocument1 pageNew Microsoft Word DocumentNarinder GautamNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Content ServerDocument11 pagesContent ServerNarinder GautamNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Progress: The L'Oréal Sustainability CommitmentDocument28 pagesProgress: The L'Oréal Sustainability CommitmentNarinder GautamNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- New Microsoft Word DocumentDocument1 pageNew Microsoft Word DocumentNarinder GautamNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- GMLC - Round 1 Market AnalysisDocument4 pagesGMLC - Round 1 Market AnalysisNarinder GautamNo ratings yet
- SOM Handwritten Notes PDFDocument25 pagesSOM Handwritten Notes PDFNarinder GautamNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Ko Wai Ahau?: Name: Job Title: Whatidointh Is JobDocument1 pageKo Wai Ahau?: Name: Job Title: Whatidointh Is JobNarinder GautamNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Analysis of Landuse PlansDocument6 pagesAnalysis of Landuse PlansNarinder GautamNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- A Flexible Policy Framework For Analysing Multimodal Freight Transportation System in India: SAP-LAP and Efficient IRP MethodDocument18 pagesA Flexible Policy Framework For Analysing Multimodal Freight Transportation System in India: SAP-LAP and Efficient IRP MethodNarinder GautamNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- EaljfhoDocument2 pagesEaljfhoNarinder GautamNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Welcome To The R Eal Game: Nau Mai Ki Te Ke-Mu Tu-TuruDocument1 pageWelcome To The R Eal Game: Nau Mai Ki Te Ke-Mu Tu-TuruNarinder GautamNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Supply Chain Study of Orange in JaipurDocument21 pagesSupply Chain Study of Orange in JaipurNarinder GautamNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Ipod PDFDocument4 pagesIpod PDFNarinder GautamNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Ipod PDFDocument4 pagesIpod PDFNarinder GautamNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Asdfghjkl GKHFDK, Khutesxbm KJHMDocument1 pageAsdfghjkl GKHFDK, Khutesxbm KJHMNarinder GautamNo ratings yet
- 5 - 1 Deflection of Beams PDFDocument8 pages5 - 1 Deflection of Beams PDFsaurabh shuklaNo ratings yet
- Academic Calendar 2016-17 Odd and Even SemDocument4 pagesAcademic Calendar 2016-17 Odd and Even SemGaurav Kumar BadhotiyaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- New Text DocumentDocument1 pageNew Text DocumentNarinder GautamNo ratings yet
- Mechanical Measurement and Control System Unit 1: Code: Credit: 04 L-T-P: (3-1-0)Document1 pageMechanical Measurement and Control System Unit 1: Code: Credit: 04 L-T-P: (3-1-0)Narinder GautamNo ratings yet
- 18Document3 pages18Narinder GautamNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Story Is Such A Great Work of HonouerDocument1 pageThe Story Is Such A Great Work of HonouerNarinder GautamNo ratings yet
- Basic Concepts of Strength of MaterialsDocument50 pagesBasic Concepts of Strength of Materialsmegharajamds93% (29)
- Chere Wealiya Soheneyas Rok Gaddi Ve Jaana Dur Ve Pardesi Mahi Aty (Po AhipujbDocument1 pageChere Wealiya Soheneyas Rok Gaddi Ve Jaana Dur Ve Pardesi Mahi Aty (Po AhipujbNarinder GautamNo ratings yet
- Pavni Boss ComplaintsDocument1 pagePavni Boss ComplaintsNarinder GautamNo ratings yet
- Guns On RosesDocument1 pageGuns On RosesNarinder GautamNo ratings yet
- 2week Menu Jan 2015Document1 page2week Menu Jan 2015Narinder GautamNo ratings yet
- Twogether Article 25 en 62Document2 pagesTwogether Article 25 en 62BiantoroKunartoNo ratings yet
- A Modelling Study of Metal Cutting With Abrasive WaterjetDocument13 pagesA Modelling Study of Metal Cutting With Abrasive WaterjetАО НИИТ АО НИИТNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- 008-003-KUC-Guia para Medicion de CarrileriaDocument211 pages008-003-KUC-Guia para Medicion de CarrileriaYerk ManNo ratings yet
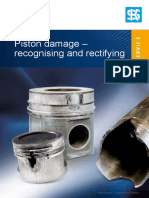
- Piston Damage - Recognising and RectifyingDocument108 pagesPiston Damage - Recognising and RectifyingFalgon IslamNo ratings yet
- GT Drilling Bits 6aug FinalDocument46 pagesGT Drilling Bits 6aug FinalRanjith Premadasan100% (1)
- Machine Design FundamentalsDocument54 pagesMachine Design FundamentalsPramod ShriwastavaNo ratings yet
- Review For Development of Hydraulic Excavator Attachment: YANG Cheng Huang Kui LI Yinwu WANG Jingchun ZHOU MengDocument5 pagesReview For Development of Hydraulic Excavator Attachment: YANG Cheng Huang Kui LI Yinwu WANG Jingchun ZHOU MengZuhaib ShaikhNo ratings yet
- Tribology BasicsDocument89 pagesTribology BasicsManjunath GowdaNo ratings yet
- C1138M-12 Standard Test Method For Abrasion Resistance of Concrete (Underwater Method) PDFDocument5 pagesC1138M-12 Standard Test Method For Abrasion Resistance of Concrete (Underwater Method) PDFbilal natherNo ratings yet
- A 02110113Document13 pagesA 02110113AJER JOURNALNo ratings yet
- Croda Stick em InglesDocument24 pagesCroda Stick em InglesMichelle Fernanda Silva FerrazNo ratings yet
- 10 5923 J Ijmee 20120106 04Document5 pages10 5923 J Ijmee 20120106 04SafetyanaNo ratings yet
- Chapter 3 TYPICAL DAMAGES OF MACHINE PARTSDocument19 pagesChapter 3 TYPICAL DAMAGES OF MACHINE PARTSOusman ToficNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Habasit Chain Engineering GuideDocument62 pagesHabasit Chain Engineering GuideScripts TeamNo ratings yet
- Epoxy Catalogue 2007 PDFDocument24 pagesEpoxy Catalogue 2007 PDFbreno_gcNo ratings yet
- Office furniture testing standards BIFMA ANSIDocument5 pagesOffice furniture testing standards BIFMA ANSIRitesh BijawatNo ratings yet
- 250 RIMERA en Book Print MiniDocument78 pages250 RIMERA en Book Print Miniaristi51No ratings yet
- RTB 1 04b Bearing Designs TBUDocument14 pagesRTB 1 04b Bearing Designs TBUmatrix2525009100% (1)
- ASB 429-19-50 Page 1 of 9 Approved For Public ReleaseDocument9 pagesASB 429-19-50 Page 1 of 9 Approved For Public Releaserio tanoneNo ratings yet
- Astm D4060-10Document5 pagesAstm D4060-10Diomer Alzate Berrio100% (1)
- Bisalloy Tech Guide 2012-2013Document100 pagesBisalloy Tech Guide 2012-2013Edwards RayNo ratings yet
- Abuse-Resistant Nondecorated Interior Gypsum Panel Products and Fiber-Reinforced Cement PanelsDocument7 pagesAbuse-Resistant Nondecorated Interior Gypsum Panel Products and Fiber-Reinforced Cement PanelsINARQ1979No ratings yet
- Engine Bearing Fundamentals: Lubrication FilmDocument2 pagesEngine Bearing Fundamentals: Lubrication Filmeng_ebrahim_2000No ratings yet
- DEVA Metal Manual enDocument24 pagesDEVA Metal Manual ennfcastingsNo ratings yet
- En 41Document1 pageEn 41Traveller RawatNo ratings yet
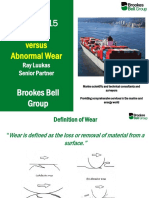
- Ray LuukasDocument35 pagesRay LuukasThe SMNo ratings yet
- Abrasive and Adhesive Wear Behaviour of Metallic Bonds in A Syntheti - 2021 - WeDocument8 pagesAbrasive and Adhesive Wear Behaviour of Metallic Bonds in A Syntheti - 2021 - WeEdsonNo ratings yet
- Nilos MatDocument8 pagesNilos MatMohd NazriNo ratings yet
- Introduccion Al SRM ATR72Document60 pagesIntroduccion Al SRM ATR72Daniel Hernandez100% (1)
- 130180708005-Experimental Investigation of Cutting Force and Tool Wear Behaviour While Dry Turning Inconel 625Document106 pages130180708005-Experimental Investigation of Cutting Force and Tool Wear Behaviour While Dry Turning Inconel 625Chaudhari HileshNo ratings yet
- Piping and Pipeline Calculations Manual: Construction, Design Fabrication and ExaminationFrom EverandPiping and Pipeline Calculations Manual: Construction, Design Fabrication and ExaminationRating: 4 out of 5 stars4/5 (18)
- Nuclear Energy in the 21st Century: World Nuclear University PressFrom EverandNuclear Energy in the 21st Century: World Nuclear University PressRating: 4.5 out of 5 stars4.5/5 (3)
- Functional Safety from Scratch: A Practical Guide to Process Industry ApplicationsFrom EverandFunctional Safety from Scratch: A Practical Guide to Process Industry ApplicationsNo ratings yet
- An Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksFrom EverandAn Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksRating: 5 out of 5 stars5/5 (1)
- Chemical Process Safety: Learning from Case HistoriesFrom EverandChemical Process Safety: Learning from Case HistoriesRating: 4 out of 5 stars4/5 (14)