You might also like
- FlashcardsDocument18 pagesFlashcardsDaphne HernaezNo ratings yet
- Instructions For Senior High School ApplicantsDocument2 pagesInstructions For Senior High School ApplicantsDaphne HernaezNo ratings yet
- Bchm3300 P2 MCDocument11 pagesBchm3300 P2 MCDaphne HernaezNo ratings yet
- LipidsDocument3 pagesLipidsTenshi Kathzka AgcaoiliNo ratings yet
- New Microsoft Office PowerPoint PresentationDocument1 pageNew Microsoft Office PowerPoint PresentationGbsReddyNo ratings yet
- Passport Applicationform 2015Document2 pagesPassport Applicationform 2015genesisrdomingoNo ratings yet
- Evangelical PovertyDocument4 pagesEvangelical PovertyDaphne HernaezNo ratings yet
- Board Border 2016Document6 pagesBoard Border 2016Daphne HernaezNo ratings yet
- z2 Amphetamines and EcstasyDocument2 pagesz2 Amphetamines and EcstasyDaphne HernaezNo ratings yet
- Hard CC Hard CC Hard CC Hard CCDocument2 pagesHard CC Hard CC Hard CC Hard CCDaphne HernaezNo ratings yet
- Cannabinoids - Structures, Effects, and ClassificationDocument19 pagesCannabinoids - Structures, Effects, and ClassificationDaphne HernaezNo ratings yet
- Cannabinoid ReportDocument14 pagesCannabinoid ReportDaphne HernaezNo ratings yet
- Top 10 Benefits of CannabisDocument7 pagesTop 10 Benefits of CannabisDaphne HernaezNo ratings yet
- Top 10 Benefits of CannabisDocument1 pageTop 10 Benefits of CannabisDaphne HernaezNo ratings yet
- HaematologyDocument37 pagesHaematologyDaphne HernaezNo ratings yet
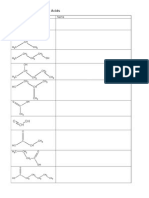
- Alcohol and Carboxylic AcidsDocument2 pagesAlcohol and Carboxylic AcidsJose Barrera GaleraNo ratings yet
- The Clinical Role of Genetic Polymorphisms in DrugDocument2 pagesThe Clinical Role of Genetic Polymorphisms in DrugDaphne HernaezNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Discursive EssayDocument2 pagesDiscursive EssaySara100% (1)
- IntroductionDocument12 pagesIntroductionpeterjongNo ratings yet
- Pertussis Whooping Cough Letter To ParentsDocument1 pagePertussis Whooping Cough Letter To ParentsPiper Garner RiddleNo ratings yet
- Diphtheria, Tetanus, Pertussis (Dtap) VaccineDocument4 pagesDiphtheria, Tetanus, Pertussis (Dtap) VaccinePromise EncinaresNo ratings yet
- Template Argumentative Essay-Writing IiiDocument7 pagesTemplate Argumentative Essay-Writing Iiierina rosantiNo ratings yet
- Tragic Choices MMR-austism Case Study In-Class VersionDocument64 pagesTragic Choices MMR-austism Case Study In-Class VersionMichael McIntoshNo ratings yet
- Inform The Benefits of Breast Feeding To Mother and BabbiesDocument11 pagesInform The Benefits of Breast Feeding To Mother and BabbiesZulfhi WahyuniNo ratings yet
- Answers To Mike Adams's 21 Curious Questions About VaccinesDocument32 pagesAnswers To Mike Adams's 21 Curious Questions About VaccinesLiz DitzNo ratings yet
- 1.national Guide To A Preventive Health Assessment For Aboriginal and Torres Strait Islander PeopleDocument100 pages1.national Guide To A Preventive Health Assessment For Aboriginal and Torres Strait Islander PeopleRumana AliNo ratings yet
- Paediatrica Indonesiana: Fadilah Harahap, Ridwan M. Daulay, Muhammad Ali, Wisman Dalimunthe, Rini Savitri DaulayDocument11 pagesPaediatrica Indonesiana: Fadilah Harahap, Ridwan M. Daulay, Muhammad Ali, Wisman Dalimunthe, Rini Savitri DaulayMuhammadImamNo ratings yet
- General ChemistryDocument2 pagesGeneral ChemistryBryan Philip BejeranoNo ratings yet
- Expanded Program On ImmunizationDocument4 pagesExpanded Program On ImmunizationKrizle AdazaNo ratings yet
- 4 - Guidelines For HIV Care and Treatment in Infants and ChildrenDocument136 pages4 - Guidelines For HIV Care and Treatment in Infants and Childreniman_kundu2007756100% (1)
- NSA Bahrain Welcome Aboard 2019Document36 pagesNSA Bahrain Welcome Aboard 2019A McCormickNo ratings yet
- Dengue VirusDocument14 pagesDengue VirusditoNo ratings yet
- Administration of Injections PresentationsDocument30 pagesAdministration of Injections PresentationsgopusankarNo ratings yet
- Microbiology PDFDocument103 pagesMicrobiology PDFmedpgnotesNo ratings yet
- Adam J. Bello: Monroe County ExecutiveDocument2 pagesAdam J. Bello: Monroe County ExecutiveAdam PenaleNo ratings yet
- PW - PL - Catalogue 2009-10 PDFDocument84 pagesPW - PL - Catalogue 2009-10 PDFnawabk_26No ratings yet
- Penicillin PharmacologyDocument8 pagesPenicillin Pharmacologygulshan araNo ratings yet
- Human Development and Human BehaviorDocument11 pagesHuman Development and Human BehaviormirtchNo ratings yet
- Table 5.4.4 Water Borne Diseases Cases and Deaths (Rotavirus 2015)Document2 pagesTable 5.4.4 Water Borne Diseases Cases and Deaths (Rotavirus 2015)Al Patrick Dela CalzadaNo ratings yet
- Vaccines By: Muhammad Haikal Bin Abd RahmanDocument3 pagesVaccines By: Muhammad Haikal Bin Abd RahmanMUHAMMAD HAIKALNo ratings yet
- Nhs Covid Pass - Vaccinated: Pfizer/Biontech Covid-19 Vaccine Pfizer/Biontech Covid-19 VaccineDocument1 pageNhs Covid Pass - Vaccinated: Pfizer/Biontech Covid-19 Vaccine Pfizer/Biontech Covid-19 VaccineAnca IroaiaNo ratings yet
- Chapter 18 Vaccines and Sera - StudentDocument27 pagesChapter 18 Vaccines and Sera - StudentKumarswamy BNo ratings yet
- EPI Schedule of PakistanDocument1 pageEPI Schedule of Pakistanksbabar100% (1)
- Hypersensitivity ReactionsDocument11 pagesHypersensitivity ReactionsMenly SusadaNo ratings yet
- Notovirus InformationDocument3 pagesNotovirus InformationBrian HamiltonNo ratings yet
- Timeline-Statements of Gov't Officials On PSG VaccinationDocument2 pagesTimeline-Statements of Gov't Officials On PSG VaccinationVERA FilesNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsShristi GuptaNo ratings yet