You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 5 Kitchen Spices Ebook by Kami McbrideDocument11 pages5 Kitchen Spices Ebook by Kami Mcbridenicolas0danek100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Cell Tower Radiation Report - Sent To DOT (Department of Telecommunications)Document50 pagesCell Tower Radiation Report - Sent To DOT (Department of Telecommunications)Neha Kumar100% (9)
- Abnormalities of The PulpDocument3 pagesAbnormalities of The PulpCyril Almario Cunanan100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Biology of Tooth MovementDocument116 pagesBiology of Tooth MovementSankhya100% (1)
- Concept of OcclusionDocument81 pagesConcept of Occlusionchawalito27100% (1)
- Operational K9 TECC Challenges White Paper Final Dated 29 Sep 2015Document23 pagesOperational K9 TECC Challenges White Paper Final Dated 29 Sep 2015Maikol FloresNo ratings yet
- MYOFUNCTIONAL APPLIANCES: AN OVERVIEWDocument70 pagesMYOFUNCTIONAL APPLIANCES: AN OVERVIEWSankhya50% (2)
- Mandibular MovementsDocument140 pagesMandibular MovementsVishal Reddy100% (1)
- Feng Shui Divination Qi Men Dun Jia From The Feng Shui InstituteDocument7 pagesFeng Shui Divination Qi Men Dun Jia From The Feng Shui InstituteKiyanka Nastya100% (2)
- 1st Periodical Test Grade 9Document5 pages1st Periodical Test Grade 9Nhoj Kram Alitnacnosalliv80% (51)
- CV-Prof-MulyadiDocument69 pagesCV-Prof-MulyadityesNo ratings yet
- Doctor List at AvdDocument1 pageDoctor List at AvdSankhyaNo ratings yet
- Draft Mental Health Care Act, 2010Document43 pagesDraft Mental Health Care Act, 2010purkantiNo ratings yet
- Arnett AnalysisDocument2 pagesArnett AnalysisSankhyaNo ratings yet
- Case NumberDocument1 pageCase NumberSankhyaNo ratings yet
- 10.1016@S1072 34711590018 4Document1 page10.1016@S1072 34711590018 4SankhyaNo ratings yet
- 10.1016@S1072 34711590018 4Document1 page10.1016@S1072 34711590018 4SankhyaNo ratings yet
- JPediatrDent311-3912848 105208Document7 pagesJPediatrDent311-3912848 105208SankhyaNo ratings yet
- THE Relation OF Orthodontia TO Dentistry.Document5 pagesTHE Relation OF Orthodontia TO Dentistry.SankhyaNo ratings yet
- Amar Bhitoro Bahire Ontore OntoreDocument1 pageAmar Bhitoro Bahire Ontore OntoreSankhyaNo ratings yet
- 10.1016@S1072 34711590019 6Document11 pages10.1016@S1072 34711590019 6SankhyaNo ratings yet
- Hecker 1915Document12 pagesHecker 1915SankhyaNo ratings yet
- (Dental Summary) - It: Paeventlon of Malocclusion. (BDocument2 pages(Dental Summary) - It: Paeventlon of Malocclusion. (BSankhyaNo ratings yet
- The International Journal of Orthodontia.: Malocclusion and Mouth-Breathing.Document4 pagesThe International Journal of Orthodontia.: Malocclusion and Mouth-Breathing.SankhyaNo ratings yet
- Robinson 1915Document14 pagesRobinson 1915SankhyaNo ratings yet
- Weinberger 1915Document8 pagesWeinberger 1915SankhyaNo ratings yet
- Real Estate Act Regulation ExplainedDocument37 pagesReal Estate Act Regulation ExplainedkalaamolNo ratings yet
- The International Journal of Orthodontia.: Mastication and Food Utilization. - AgainDocument2 pagesThe International Journal of Orthodontia.: Mastication and Food Utilization. - AgainSankhyaNo ratings yet
- NOC Common Dish - Avidipta HIGDocument2 pagesNOC Common Dish - Avidipta HIGSankhyaNo ratings yet
- Orthognathic TreatmentDocument29 pagesOrthognathic TreatmentSankhyaNo ratings yet
- 10.1016@S1072 34711590022 6Document4 pages10.1016@S1072 34711590022 6SankhyaNo ratings yet
- Application For Individual MebershipDocument5 pagesApplication For Individual MebershipSankhyaNo ratings yet
- Agenda Points With BP - 9th Mar 17Document2 pagesAgenda Points With BP - 9th Mar 17SankhyaNo ratings yet
- Rare PhotographsDocument30 pagesRare PhotographsSankhya100% (1)
- General Terms & ConditionsDocument11 pagesGeneral Terms & ConditionsSankhyaNo ratings yet
- Calander 1424 Final On 8-3-2017Document14 pagesCalander 1424 Final On 8-3-2017SankhyaNo ratings yet
- NOC Common Dish - Avidipta HIGDocument2 pagesNOC Common Dish - Avidipta HIGSankhyaNo ratings yet
- 28 Jan 2016 130451497MIDC9A4GAdditionalInformationDocument84 pages28 Jan 2016 130451497MIDC9A4GAdditionalInformationSankhyaNo ratings yet
- Handbook of Poultry DiseasesDocument22 pagesHandbook of Poultry DiseasesSoufian CherkiNo ratings yet
- CalculusDocument7 pagesCalculusFaikar Ardhan ArganagaraNo ratings yet
- Getting Out of ItDocument36 pagesGetting Out of ItNavneet ChaubeyNo ratings yet
- Study Questions: CHAPTER 8 Microscopic Examination of Urine SedimentDocument7 pagesStudy Questions: CHAPTER 8 Microscopic Examination of Urine SedimentTiara YantaNo ratings yet
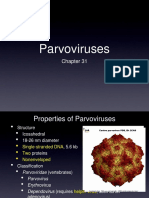
- Parvoviruses: Structure, Replication, DiseasesDocument8 pagesParvoviruses: Structure, Replication, DiseasesAldila safitriNo ratings yet
- SPJ Kelas Ibu Hamil AprilDocument20 pagesSPJ Kelas Ibu Hamil AprilHeidy AgustinaNo ratings yet
- Reproductive Systems A. B. C. DDocument6 pagesReproductive Systems A. B. C. DJamie BagundolNo ratings yet
- Health Declaration Form: (Buong Pangalan) (Petsa) (Oras) (Kasa/ukuyang Tirahan) : (Numero NG Telepono)Document1 pageHealth Declaration Form: (Buong Pangalan) (Petsa) (Oras) (Kasa/ukuyang Tirahan) : (Numero NG Telepono)Reichmond LegaspiNo ratings yet
- Abdominal Mass Differential PresentationDocument42 pagesAbdominal Mass Differential Presentationdeb haartNo ratings yet
- Oral RevalidaDocument98 pagesOral RevalidaJay ArNo ratings yet
- 1 Fluid and ElectrolyteDocument51 pages1 Fluid and ElectrolyteSanjiv SharmaNo ratings yet
- Clinical Significance Blood Group AntibodiesDocument8 pagesClinical Significance Blood Group AntibodiesSudeep RathoreNo ratings yet
- Backyard Cattle-BAKA RaisingDocument4 pagesBackyard Cattle-BAKA RaisingJessielito P. AmadorNo ratings yet
- AnemiaDocument2 pagesAnemiadianaNo ratings yet
- GGL Pelvis DelimitareDocument12 pagesGGL Pelvis DelimitareStefan AnaNo ratings yet
- The Effectiveness of Makahiya (Mimosa Pudica) Leaves Extract As An Alternative Ovicide Against Dengue Mosquito (Aedes Aegypti) EggsDocument6 pagesThe Effectiveness of Makahiya (Mimosa Pudica) Leaves Extract As An Alternative Ovicide Against Dengue Mosquito (Aedes Aegypti) EggsIya Necole GuimaryNo ratings yet
- CBC Reference Ranges by Age and GenderDocument6 pagesCBC Reference Ranges by Age and GenderbhatubimNo ratings yet
- Improving Goat Production in The Tropics: A Manual For Development WorkersDocument22 pagesImproving Goat Production in The Tropics: A Manual For Development WorkersOxfamNo ratings yet
- AssDocument54 pagesAssilmiah neuro unpadNo ratings yet
- Hemorrhoids and Anal Fissures: Causes, Symptoms and TreatmentsDocument4 pagesHemorrhoids and Anal Fissures: Causes, Symptoms and TreatmentsSanthu SuNo ratings yet
- Ayurveda Physical BodyDocument11 pagesAyurveda Physical BodyanantNo ratings yet