You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
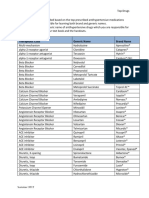
- Top Antihypertensive Drugs Generic-Brand Names PDFDocument1 pageTop Antihypertensive Drugs Generic-Brand Names PDFvidbala0% (1)
- Chapter 32 SupplementalDocument6 pagesChapter 32 SupplementalMarryNo ratings yet
- Pharma Parenteral Dosage CalculationDocument3 pagesPharma Parenteral Dosage CalculationMaxinne RoseñoNo ratings yet
- Drug Master FileDocument19 pagesDrug Master FileRenaldy NongbetNo ratings yet
- Apixaban Eliquis MonographDocument14 pagesApixaban Eliquis MonographTran Minh NgocNo ratings yet
- Obat IFARSDocument5 pagesObat IFARSOky Spinola IdroosNo ratings yet
- Laporan Permintaan Dan Lembaran Pemakaian ObatDocument12 pagesLaporan Permintaan Dan Lembaran Pemakaian ObatBunda AiniNo ratings yet
- PCEP-PC Module 4 (Pain) Solutions To Case ProblemsDocument4 pagesPCEP-PC Module 4 (Pain) Solutions To Case ProblemsMan MedNo ratings yet
- Medsurg Nursing Medications Cheat Sheet: by ViaDocument2 pagesMedsurg Nursing Medications Cheat Sheet: by ViaABEGAIL SARASUANo ratings yet
- D 5 LRDocument2 pagesD 5 LRDianelie BacenaNo ratings yet
- Tapering BenzodiazepinesDocument3 pagesTapering BenzodiazepineslgiuzfgukuzfglufzNo ratings yet
- Pedia 2Document4 pagesPedia 2John Christopher LucesNo ratings yet
- FDA Inspection Status of The SitesDocument4 pagesFDA Inspection Status of The SitesSrinivas EtikalaNo ratings yet
- TIVA Clinical Application FRCADocument4 pagesTIVA Clinical Application FRCAAmay SinghNo ratings yet
- DISPOSALDocument3 pagesDISPOSALteklil tiganiNo ratings yet
- PT - Kinarya Semesta GemilangDocument27 pagesPT - Kinarya Semesta GemilangAiko Cheryl SalsabilaNo ratings yet
- Drug Arrest ActivityDocument1 pageDrug Arrest ActivityFLNRNo ratings yet
- Rekapitulasi Laporan Narkotika: NO Nama Satuan Stok Awal Pemasukan PBFDocument10 pagesRekapitulasi Laporan Narkotika: NO Nama Satuan Stok Awal Pemasukan PBFMiftah JannahNo ratings yet
- Regulatory Requirements For Approval of Over The Counter Drugs As Per Austrailian (Tga) GuidelinesDocument23 pagesRegulatory Requirements For Approval of Over The Counter Drugs As Per Austrailian (Tga) GuidelinesBaru Chandrasekhar RaoNo ratings yet
- Sinarest AF SyrupDocument5 pagesSinarest AF SyrupImshan TalibNo ratings yet
- Review-Optimal Use of Benda-2015Document18 pagesReview-Optimal Use of Benda-2015abdullahNo ratings yet
- Inactive Ingredient Search CarbomerDocument5 pagesInactive Ingredient Search CarbomerRicardo Alonso Abril RamírezNo ratings yet
- 318746Document16 pages318746Douglas Obrahiam ShawcroftNo ratings yet
- Astrazenica 2nd Dose 8-13-21 AlkieDocument109 pagesAstrazenica 2nd Dose 8-13-21 AlkieGanie Mar BiasonNo ratings yet
- Fda AmoxicillinDocument18 pagesFda AmoxicillingitapusNo ratings yet
- HTN Protocol 6.05Document2 pagesHTN Protocol 6.05Sergiu CiurdariuNo ratings yet
- Marijuana and DUI Laws PDFDocument3 pagesMarijuana and DUI Laws PDFJake B EllisonNo ratings yet
- Oritavancin Orbactiv MonographDocument11 pagesOritavancin Orbactiv MonographDani11No ratings yet
- Ketorolac Tromethamine Tablet PDFDocument5 pagesKetorolac Tromethamine Tablet PDFrabd samNo ratings yet
- Maxlax - Marketing PlanDocument26 pagesMaxlax - Marketing PlanaamirNo ratings yet