You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- EPA Section 608 Type I Open Book ManualDocument148 pagesEPA Section 608 Type I Open Book ManualMehdi AbbasNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Cracks and Fractures in TeethDocument6 pagesCracks and Fractures in Teethizeldien5870No ratings yet
- Company Registration Procedure Handbook in Cambodia, EnglishDocument124 pagesCompany Registration Procedure Handbook in Cambodia, EnglishThea100% (16)
- Master TutorialDocument95 pagesMaster TutorialWackyWabbit0% (1)
- Microbiological Quality Ice CreamDocument9 pagesMicrobiological Quality Ice CreamocortezlariosNo ratings yet
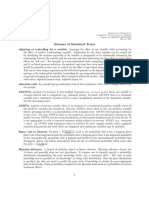
- Glossary of Statistical Terms: Roger Stern, Ian Dale and Sandro LeidiDocument23 pagesGlossary of Statistical Terms: Roger Stern, Ian Dale and Sandro Leidiizeldien5870No ratings yet
- Australian Dental Journal Style GuideDocument7 pagesAustralian Dental Journal Style Guideizeldien5870No ratings yet
- The Success of Endodontic Therapy Healing and Functionality Friedman PDFDocument11 pagesThe Success of Endodontic Therapy Healing and Functionality Friedman PDFizeldien5870No ratings yet
- Philpost RRDocument6 pagesPhilpost RRGene AbotNo ratings yet
- LET-English-Structure of English-ExamDocument57 pagesLET-English-Structure of English-ExamMarian Paz E Callo80% (5)
- Advice Sheet A12 - Infection Control in Dentistry - Identist - 2 PDFDocument31 pagesAdvice Sheet A12 - Infection Control in Dentistry - Identist - 2 PDFizeldien5870No ratings yet
- Mechanisms and Risk Factors For Fracture Prediliction of Endodontically Treated Teeth ANIL KISHENDocument27 pagesMechanisms and Risk Factors For Fracture Prediliction of Endodontically Treated Teeth ANIL KISHENizeldien5870100% (1)
- Leibniz, Gottfried Wilhelm - Strickland, Lloyd - Leibniz's Monadology - A New Translation and Guide-Edinburgh University Press (2014)Document327 pagesLeibniz, Gottfried Wilhelm - Strickland, Lloyd - Leibniz's Monadology - A New Translation and Guide-Edinburgh University Press (2014)Gigla Gonashvili100% (1)
- Hydrogen Production by Steam ReformingDocument10 pagesHydrogen Production by Steam ReformingramiarenasNo ratings yet
- Cone Beam Computed Tomography (CBCT) in EndodonticsDocument7 pagesCone Beam Computed Tomography (CBCT) in Endodonticsizeldien5870No ratings yet
- Handbook Systematic ReviewsDocument56 pagesHandbook Systematic Reviewsizeldien5870No ratings yet
- An Introduction To MetaanalysisDocument10 pagesAn Introduction To MetaanalysisJaimeNo ratings yet
- Introduction To Systematic Reviews PowerpointDocument30 pagesIntroduction To Systematic Reviews Powerpointizeldien5870No ratings yet
- Minimally Invasive Endodontics A Promising Future Concept A Review Article - 2017Document7 pagesMinimally Invasive Endodontics A Promising Future Concept A Review Article - 2017izeldien5870No ratings yet
- Combining Effect Size Estimates in Meta-Analysis WithDocument21 pagesCombining Effect Size Estimates in Meta-Analysis Withizeldien5870No ratings yet
- Getting Started With Meta-Analysis PDFDocument10 pagesGetting Started With Meta-Analysis PDFizeldien5870No ratings yet
- An Introduction To Meta-Analysis2014 PDFDocument8 pagesAn Introduction To Meta-Analysis2014 PDFThalia KarampasiNo ratings yet
- Part 1 Preparing For Meta-Analysis 2016Document41 pagesPart 1 Preparing For Meta-Analysis 2016izeldien5870No ratings yet
- Learning Statistics With R PDFDocument616 pagesLearning Statistics With R PDFAnonymNo ratings yet
- Biomechanical Considerations For The Restoration On Endodontically Treated Teeth. A Systematic Review of The Literature-Part I. Composition and Micro and Macrostructure AlterationsDocument11 pagesBiomechanical Considerations For The Restoration On Endodontically Treated Teeth. A Systematic Review of The Literature-Part I. Composition and Micro and Macrostructure AlterationsGonzalo Bravo Ahumada100% (1)
- Modern Anterior Endodontic Access and Directed Dentin Conservation David Clark & John Khademi PDFDocument5 pagesModern Anterior Endodontic Access and Directed Dentin Conservation David Clark & John Khademi PDFizeldien5870No ratings yet
- Toronto-Study Phase 1 Initial TreatmentDocument7 pagesToronto-Study Phase 1 Initial Treatmentizeldien5870No ratings yet
- Biomechanical Considerations For The Restoration On Endodontically Treated Teeth. A Systematic Review of The Literature-Part I. Composition and Micro and Macrostructure AlterationsDocument11 pagesBiomechanical Considerations For The Restoration On Endodontically Treated Teeth. A Systematic Review of The Literature-Part I. Composition and Micro and Macrostructure AlterationsGonzalo Bravo Ahumada100% (1)
- Minimally Invasive Endodontics Challenging Prevailing ParadigmsDocument7 pagesMinimally Invasive Endodontics Challenging Prevailing Paradigmsizeldien5870No ratings yet
- Modern AccessDocument25 pagesModern AccesstapobarnaNo ratings yet
- Minimally InvasiveDocument2 pagesMinimally InvasiveShipra SinghNo ratings yet
- How To Estimate and Interpret Various Effect SizesDocument9 pagesHow To Estimate and Interpret Various Effect Sizesizeldien5870No ratings yet
- GlossaryDocument38 pagesGlossaryizeldien5870No ratings yet
- GlossaryDocument14 pagesGlossaryechofox11No ratings yet
- Study Design in Medical ResearchDocument6 pagesStudy Design in Medical Researchizeldien5870No ratings yet
- Bite Force References From TextbooksDocument2 pagesBite Force References From Textbooksizeldien5870No ratings yet
- The Tyranny of PowerDocument8 pagesThe Tyranny of Powerizeldien5870No ratings yet
- 04 Membrane Structure NotesDocument22 pages04 Membrane Structure NotesWesley ChinNo ratings yet
- Evaporative CoolingDocument68 pagesEvaporative Coolingshivas34regal100% (1)
- RseDocument60 pagesRseH S Vishwanath ShastryNo ratings yet
- Atoll 1400Document2 pagesAtoll 1400David M. SeoaneNo ratings yet
- MSDS Formic AcidDocument3 pagesMSDS Formic AcidChirag DobariyaNo ratings yet
- Purification of Dilactide by Melt CrystallizationDocument4 pagesPurification of Dilactide by Melt CrystallizationRaj SolankiNo ratings yet
- EvolutionCombatMedic 2022Document17 pagesEvolutionCombatMedic 2022smith.kevin1420344100% (1)
- Measuring and Modeling Vertical Crosshead Vibration in Api-618 Reciprocating CompressorsDocument18 pagesMeasuring and Modeling Vertical Crosshead Vibration in Api-618 Reciprocating CompressorshmshawkiNo ratings yet
- PUPiApplyVoucher2017 0006 3024Document2 pagesPUPiApplyVoucher2017 0006 3024MätthëwPïńëdäNo ratings yet
- 377 Situational Expression Advanced Level Test Quiz Online Exercise With Answers 1Document7 pages377 Situational Expression Advanced Level Test Quiz Online Exercise With Answers 1zdravkamajkicNo ratings yet
- Sinamics g120p Cabinet Catalog d35 en 2018Document246 pagesSinamics g120p Cabinet Catalog d35 en 2018Edgar Lecona MNo ratings yet
- Teambinder Product BrochureDocument7 pagesTeambinder Product BrochurePrinceNo ratings yet
- Crusader Castle Al-Karak Jordan Levant Pagan Fulk, King of Jerusalem MoabDocument3 pagesCrusader Castle Al-Karak Jordan Levant Pagan Fulk, King of Jerusalem MoabErika CalistroNo ratings yet
- Service Letter Service Letter Service Letter Service Letter: Commercial Aviation ServicesDocument3 pagesService Letter Service Letter Service Letter Service Letter: Commercial Aviation ServicesSamarNo ratings yet
- Issue15 - Chirag JiyaniDocument6 pagesIssue15 - Chirag JiyaniDipankar SâháNo ratings yet
- Multi-Media Approach To Teaching-LearningDocument8 pagesMulti-Media Approach To Teaching-LearningswethashakiNo ratings yet
- NCDC-2 Physical Health Inventory Form A4Document6 pagesNCDC-2 Physical Health Inventory Form A4knock medinaNo ratings yet
- Xii Mathematics CH 01 Question BankDocument10 pagesXii Mathematics CH 01 Question BankBUNNY GOUDNo ratings yet
- HC+ Shoring System ScaffoldDocument31 pagesHC+ Shoring System ScaffoldShafiqNo ratings yet
- Coc 1 ExamDocument7 pagesCoc 1 ExamJelo BioNo ratings yet
- University of Southern Philippines Foundation. College of Engineering and ArchitectureDocument7 pagesUniversity of Southern Philippines Foundation. College of Engineering and ArchitectureJason OwiaNo ratings yet
- 2008 Kershaw CatalogDocument38 pages2008 Kershaw CatalogDANILA MARECHEKNo ratings yet
- Medical Equipment Quality Assurance For Healthcare FacilitiesDocument5 pagesMedical Equipment Quality Assurance For Healthcare FacilitiesJorge LopezNo ratings yet