You might also like
- Physical Assessment Exam Study GuideDocument35 pagesPhysical Assessment Exam Study GuideMustaf Mohamed91% (44)
- Nugget ListDocument1 pageNugget ListmsbunnileeNo ratings yet
- Resp NotesDocument14 pagesResp NotesmsbunnileeNo ratings yet
- Icu Head To Toe AssessmentDocument3 pagesIcu Head To Toe Assessmentmsbunnilee100% (2)
- Clinical Learning ObjectivesDocument4 pagesClinical Learning ObjectivesmsbunnileeNo ratings yet
- Nurs 197 Paper PPD Cultural CareDocument1 pageNurs 197 Paper PPD Cultural CaremsbunnileeNo ratings yet
- Cupping TherapyDocument6 pagesCupping TherapymsbunnileeNo ratings yet
- Key Concepts, Chapter 16, Documenting, Reporting, Conferring, and Using InformaticsDocument4 pagesKey Concepts, Chapter 16, Documenting, Reporting, Conferring, and Using InformaticsmsbunnileeNo ratings yet
- KC Chapter 10Document4 pagesKC Chapter 10msbunnileeNo ratings yet
- NCLEX TIPS 2010 Final PDFDocument24 pagesNCLEX TIPS 2010 Final PDFmsbunnileeNo ratings yet
- Key Concepts, Chapter 20, CommunicatorDocument2 pagesKey Concepts, Chapter 20, CommunicatormsbunnileeNo ratings yet
- Assessment of Fetal Well-Being Diagnostic Tests Sheet1Document2 pagesAssessment of Fetal Well-Being Diagnostic Tests Sheet1msbunnileeNo ratings yet
- Expanded PP AsmtDocument1 pageExpanded PP AsmtmsbunnileeNo ratings yet
- Key Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthDocument4 pagesKey Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthmsbunnileeNo ratings yet
- Key Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthDocument4 pagesKey Concepts, Chapter 15, Evaluating: Critically About How Best To Evaluate The Patient's Progress Toward Valued HealthmsbunnileeNo ratings yet
- Key Concepts, Chapter 14, ImplementingDocument3 pagesKey Concepts, Chapter 14, ImplementingmsbunnileeNo ratings yet
- KC Chapter 13Document3 pagesKC Chapter 13msbunnileeNo ratings yet
- KC Chapter 06Document2 pagesKC Chapter 06msbunnileeNo ratings yet
- KC Chapter 11Document3 pagesKC Chapter 11msbunnileeNo ratings yet
- The Nursing Student's Practical Guide To Writing Care Plans by Luanne BeginDocument67 pagesThe Nursing Student's Practical Guide To Writing Care Plans by Luanne Beginsoghosa100% (1)
- KC Chapter 07Document3 pagesKC Chapter 07msbunnileeNo ratings yet
- 2016 RN Test Plan CandidateDocument61 pages2016 RN Test Plan CandidateKaren Mae Ü DonaireNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Loan Modification/Loss Mitigation Contacts and Phone Numbers ListDocument6 pagesLoan Modification/Loss Mitigation Contacts and Phone Numbers ListSteve Linnin100% (11)
- Card Payments in 2017Document1 pageCard Payments in 2017sissthwae ooNo ratings yet
- Risk and Insurance: Biyani's Think TankDocument122 pagesRisk and Insurance: Biyani's Think TankFaiz Ur RehmanNo ratings yet
- A6V11227546 enDocument142 pagesA6V11227546 enCtwoR MantenimientosNo ratings yet
- Workfile - ZCDocument25 pagesWorkfile - ZCirshadpp999iNo ratings yet
- Final Project-1Document68 pagesFinal Project-1kunju pkNo ratings yet
- UDC VerificationDocument3 pagesUDC VerificationDanielNo ratings yet
- Content Chapter I: Direct Marketing. Definition. How It Works Chapter II: DM Features. Benefits and Tools of Direct Marketing Conclusion ReferencesDocument22 pagesContent Chapter I: Direct Marketing. Definition. How It Works Chapter II: DM Features. Benefits and Tools of Direct Marketing Conclusion ReferencesCray AlisterNo ratings yet
- Account Statement For Account:2962000100457772: Branch DetailsDocument2 pagesAccount Statement For Account:2962000100457772: Branch DetailsBest Auto TechNo ratings yet
- Startups 20Document3 pagesStartups 20Rafi AzamNo ratings yet
- Audit Cendant CorpDocument23 pagesAudit Cendant CorpAjeng Feby PalupiNo ratings yet
- Solution Manual For Auditing and Assurance Services 17th Edition Alvin A Arens Randal J Elder Mark S Beasley Chris e HoganDocument31 pagesSolution Manual For Auditing and Assurance Services 17th Edition Alvin A Arens Randal J Elder Mark S Beasley Chris e HoganMeredithFleminggztay100% (79)
- MessageDocument3 pagesMessageabderahmane BebbouNo ratings yet
- Ticket LoveDocument3 pagesTicket LoveVedans FinancesNo ratings yet
- NIA PREMIUM CHART 29sept18Document1 pageNIA PREMIUM CHART 29sept18Bob KratoNo ratings yet
- Copy - 2 - of Principles of Accounting Note Year 1Document213 pagesCopy - 2 - of Principles of Accounting Note Year 1Rexford Atta-boakye JnrNo ratings yet
- Internal Audit Annual Report PWCDocument21 pagesInternal Audit Annual Report PWCarroshan100% (14)
- Theory of AccountDocument1 pageTheory of Accountzee abadilla100% (1)
- Sree Anasuya Annual Report 03-04Document22 pagesSree Anasuya Annual Report 03-04api-19728905No ratings yet
- Coffee Craft Daily Service TableDocument3 pagesCoffee Craft Daily Service TableAdlin LinaNo ratings yet
- Naukri ChandanSarkar (5y 0m)Document2 pagesNaukri ChandanSarkar (5y 0m)Babji RohitNo ratings yet
- ABA Bank: Garcia, Renz Xavier Vinluan, Jan Danniel Bañares, Zcyrelle Yvonne Salazar, Diana Mae Torres, Mhariecar AubreyDocument9 pagesABA Bank: Garcia, Renz Xavier Vinluan, Jan Danniel Bañares, Zcyrelle Yvonne Salazar, Diana Mae Torres, Mhariecar AubreyRichard Rhamil Carganillo Garcia Jr.No ratings yet
- A16 Servicing HelloGoodbye LetterDocument2 pagesA16 Servicing HelloGoodbye LetterRicharnellia-RichieRichBattiest-CollinsNo ratings yet
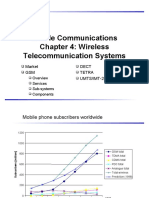
- Mobile Communications Chapter 4: Wireless Telecommunication SystemsDocument74 pagesMobile Communications Chapter 4: Wireless Telecommunication SystemsRAJESHNo ratings yet
- Statement: (Including Pots)Document3 pagesStatement: (Including Pots)13KARATNo ratings yet
- Valix Accounting Compilation Assessment KeyDocument2 pagesValix Accounting Compilation Assessment KeyCelineNo ratings yet
- Savings Account Statement: Capitec B AnkDocument8 pagesSavings Account Statement: Capitec B AnkLonwaboNo ratings yet
- Pass Issuance Receipt: Now You Can Also Buy This Pass On Paytm AppDocument1 pagePass Issuance Receipt: Now You Can Also Buy This Pass On Paytm AppAnoop SharmaNo ratings yet
- 3359-2 Zurich ValueLife Junior Brochure R2Document22 pages3359-2 Zurich ValueLife Junior Brochure R2Venodaren VelusamyNo ratings yet
- Health 101 Research PaperDocument14 pagesHealth 101 Research Paperapi-302787939No ratings yet