You might also like
- Early Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsFrom EverandEarly Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsNo ratings yet
- QC Lab Feb2018Document46 pagesQC Lab Feb2018khawar.nehalNo ratings yet
- UHC White PaperDocument26 pagesUHC White PaperArielle Winchester100% (1)
- A Checklist For Ensuring Product QualityDocument37 pagesA Checklist For Ensuring Product QualityHadera Tesfay0% (1)
- A Guide For Implementing The Approach To Build Skills For Pharmaceutical ManagementDocument95 pagesA Guide For Implementing The Approach To Build Skills For Pharmaceutical ManagementIFRS SimoNo ratings yet
- 13 173 JordanProphylaxisCesareanSection - No PptsDocument84 pages13 173 JordanProphylaxisCesareanSection - No Pptsnurul wahyuniNo ratings yet
- Session 9. Strategies To Improve Medicine Use-: Drug and Therapeutics Committee Training CourseDocument24 pagesSession 9. Strategies To Improve Medicine Use-: Drug and Therapeutics Committee Training CourseNshimiyimana Jean ClaudeNo ratings yet
- Quantification of Health Commodities - RMNCH SupplementDocument173 pagesQuantification of Health Commodities - RMNCH Supplementv_ratNo ratings yet
- Pnadp 443Document58 pagesPnadp 443parwana formuliNo ratings yet
- Quantification of Health Commodities 6-11-16 3Document174 pagesQuantification of Health Commodities 6-11-16 3yordanosezerihun07No ratings yet
- Guidelines For Donations of Medicines and Health Care Equipment in NigeriaDocument39 pagesGuidelines For Donations of Medicines and Health Care Equipment in NigerianeodvxNo ratings yet
- Medicines Promotion: Assessing The Nature, Extent and Impact of RegulationDocument38 pagesMedicines Promotion: Assessing The Nature, Extent and Impact of RegulationAsmitaNo ratings yet
- Guidelines On Pharmacovigilance 1Document20 pagesGuidelines On Pharmacovigilance 1NatashaNo ratings yet
- Bookshelf NBK578525Document98 pagesBookshelf NBK578525Lucas WillianNo ratings yet
- Bookshelf NBK578487Document170 pagesBookshelf NBK578487Lucas WillianNo ratings yet
- Essential Medicines Lists Punjab 2014Document65 pagesEssential Medicines Lists Punjab 2014Salman Nazir WattuNo ratings yet
- Criterios de Elegibilidad de ACODocument88 pagesCriterios de Elegibilidad de ACOquimegiNo ratings yet
- Pharmaceutical Quality For The 21st Century A Risk-Based Approach Progress Report - FDADocument29 pagesPharmaceutical Quality For The 21st Century A Risk-Based Approach Progress Report - FDAdoctoramermotNo ratings yet
- Pnacn 723Document44 pagesPnacn 723Nati AbebeNo ratings yet
- Pharmaco VigilanceDocument46 pagesPharmaco VigilanceBirupakshya Rout100% (1)
- SaludpreconcepcionalDocument30 pagesSaludpreconcepcionalapi-26512586No ratings yet
- Baseline Study of Private Drug Shops in Bangladesh: Findings and RecommendationsDocument57 pagesBaseline Study of Private Drug Shops in Bangladesh: Findings and Recommendationsrubana reazNo ratings yet
- OrganizationsDocument4 pagesOrganizationsDurgaNadellaNo ratings yet
- Pharmaceutical Country Profile Saint LuciaDocument97 pagesPharmaceutical Country Profile Saint Luciamanish patilNo ratings yet
- 08 National IPC Standards For Hospitals in Tanzania FinalDocument85 pages08 National IPC Standards For Hospitals in Tanzania FinalPaschal Kunambi100% (2)
- 04 PG Dug Safety Final 08Document30 pages04 PG Dug Safety Final 08romantic jannatNo ratings yet
- Pharmacovigilance: Need and Future Prospective in Herbal and Ayurvedic MedicinesDocument5 pagesPharmacovigilance: Need and Future Prospective in Herbal and Ayurvedic MedicinesBhavana GangurdeNo ratings yet
- Mrbarnes CV Jan2023Document3 pagesMrbarnes CV Jan2023api-668851426No ratings yet
- KAP Survey PDFDocument22 pagesKAP Survey PDFEssam MunirNo ratings yet
- Adi UtariniDocument72 pagesAdi UtarinitheskywlkrNo ratings yet
- U.S. Medical Eligibility Criteria For Contraceptive Use, 2010Document88 pagesU.S. Medical Eligibility Criteria For Contraceptive Use, 2010carolinaseguram707No ratings yet
- Bank Counterfeit WorkshopDocument22 pagesBank Counterfeit WorkshopMohammed AljaradiNo ratings yet
- Monitoring GuidanceDocument18 pagesMonitoring GuidanceIstvan SomogyiNo ratings yet
- Health System Profile-Honduras 2009Document57 pagesHealth System Profile-Honduras 2009dinesh sawandNo ratings yet
- PBC 2012 JCI Standards To Evaluate and Improve Pediatric Oncology Nursing Care in Guatemala PDFDocument6 pagesPBC 2012 JCI Standards To Evaluate and Improve Pediatric Oncology Nursing Care in Guatemala PDFEMIGDIO1969No ratings yet
- Final Standard Treatment Guidelines Booklet 04Document530 pagesFinal Standard Treatment Guidelines Booklet 04Mwellscribd MalitNo ratings yet
- Evaluating Drug Costs FinalDocument26 pagesEvaluating Drug Costs Finalnurhayati novitaNo ratings yet
- (3.2) WHO Prequalification Project - Status 2006Document21 pages(3.2) WHO Prequalification Project - Status 2006Jose PerezNo ratings yet
- Guideline Kontrasepsi 1Document62 pagesGuideline Kontrasepsi 1Laila Azzahrah SilitongaNo ratings yet
- Ethics Committee Accreditation Under Clinical Trial ProgramDocument24 pagesEthics Committee Accreditation Under Clinical Trial ProgramAjay ManeNo ratings yet
- Use of Ebola Vaccine: Recommendations of The Advisory Committee On Immunization Practices, United States, 2020Document16 pagesUse of Ebola Vaccine: Recommendations of The Advisory Committee On Immunization Practices, United States, 2020worksheetbookNo ratings yet
- Quality Improvement in Clinical LaboratoDocument10 pagesQuality Improvement in Clinical LaboratoJuly K - APFCB JulyK100% (1)
- Measure EmpowermentDocument48 pagesMeasure EmpowermentraysamuslimcornerNo ratings yet
- Final Drug Residues in Milk 4-26-2015Document358 pagesFinal Drug Residues in Milk 4-26-2015Vintila LiviuNo ratings yet
- Global PV Update and ImportanceDocument24 pagesGlobal PV Update and ImportanceAmeeraYoungNo ratings yet
- 10 PG Standard Treatment Guidelines Final 08Document24 pages10 PG Standard Treatment Guidelines Final 08yosafat mustikoartoNo ratings yet
- Mongolia Pharma ReportDocument38 pagesMongolia Pharma ReportphamleminhNo ratings yet
- Edward P Conway - Curriculum Vitae Seven RPHDocument3 pagesEdward P Conway - Curriculum Vitae Seven RPHEd Conway0% (1)
- Anthropometric Indicators Measurement Guide: 2003 Revised EditionDocument92 pagesAnthropometric Indicators Measurement Guide: 2003 Revised Editioncibyy_roNo ratings yet
- Guidelines For The Management of Pregnant Women With Obesity: A Systematic ReviewDocument14 pagesGuidelines For The Management of Pregnant Women With Obesity: A Systematic ReviewMichael ThomasNo ratings yet
- Primary Care 8april09Document214 pagesPrimary Care 8april09Nia RodearniNo ratings yet
- 18 002 SIAPS Benin - Technical Report - FinalDocument24 pages18 002 SIAPS Benin - Technical Report - Finalmanish patilNo ratings yet
- Pharmacovigilance Programme ofDocument4 pagesPharmacovigilance Programme ofpavani valluriNo ratings yet
- ZW Arv Therapy PreventionDocument88 pagesZW Arv Therapy PreventionOwen F MarimiraNo ratings yet
- SOGC - Endometriosis Diagnosis and ManagementDocument36 pagesSOGC - Endometriosis Diagnosis and ManagementreioctabianoNo ratings yet
- R HFA Report Example RwandaDocument66 pagesR HFA Report Example RwandaOluranti SijuwolaNo ratings yet
- Probiotic Evidence ReportDocument645 pagesProbiotic Evidence ReportThiago PessoaNo ratings yet
- Global Youth Tobacco Surveillance, 2000-2007: Morbidity and Mortality Weekly ReportDocument32 pagesGlobal Youth Tobacco Surveillance, 2000-2007: Morbidity and Mortality Weekly ReportAnisa SafutriNo ratings yet
- Regulatory Aspects of Pharmaceutical Quality System: Brief IntroductionFrom EverandRegulatory Aspects of Pharmaceutical Quality System: Brief IntroductionNo ratings yet
- Di MCB DB Pricelist01!07!2018Document1 pageDi MCB DB Pricelist01!07!2018saurabhjerps231221No ratings yet
- Definition of Sustainable Packaging PDFDocument10 pagesDefinition of Sustainable Packaging PDFProf C.S.PurushothamanNo ratings yet
- (The Nineteenth Century Series) Grace Moore - Dickens and Empire - Discourses of Class, Race and Colonialism in The Works of Charles Dickens-Routledge (2004) PDFDocument223 pages(The Nineteenth Century Series) Grace Moore - Dickens and Empire - Discourses of Class, Race and Colonialism in The Works of Charles Dickens-Routledge (2004) PDFJesica LengaNo ratings yet
- Sowk-625 Iq Tool 4Document22 pagesSowk-625 Iq Tool 4api-405320544No ratings yet
- 1 Introduction To Pharmaceutical Dosage Forms Part1Document32 pages1 Introduction To Pharmaceutical Dosage Forms Part1Joanna Carla Marmonejo Estorninos-Walker100% (1)
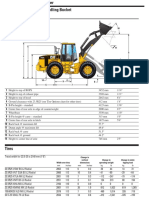
- Cat It62hDocument4 pagesCat It62hMarceloNo ratings yet
- Consolidated Companies ListDocument31 pagesConsolidated Companies ListSamir OberoiNo ratings yet
- Pivacare Preventive-ServiceDocument1 pagePivacare Preventive-ServiceSadeq NeiroukhNo ratings yet
- Fabric Technologist RoleDocument3 pagesFabric Technologist RoleAnup Kumar DeyNo ratings yet
- CH7Document34 pagesCH7Abdul AzizNo ratings yet
- Occupational Stress Questionnaire PDFDocument5 pagesOccupational Stress Questionnaire PDFabbaskhodaei666No ratings yet
- Data Sheet: Permanent Magnet GeneratorDocument2 pagesData Sheet: Permanent Magnet Generatordiegoadjgt100% (1)
- Samarth Arora: Curriculum VitaeDocument2 pagesSamarth Arora: Curriculum VitaeAditya SinghalNo ratings yet
- Juegos PPCDocument8 pagesJuegos PPCikro995No ratings yet
- What Is Bitcoin MiningDocument4 pagesWhat Is Bitcoin MiningCarmen M Leal CurielNo ratings yet
- Research On Surface Roughness by Laser CDocument5 pagesResearch On Surface Roughness by Laser CfatmirhusejniNo ratings yet
- Section 12-22, Art. 3, 1987 Philippine ConstitutionDocument3 pagesSection 12-22, Art. 3, 1987 Philippine ConstitutionKaren LabogNo ratings yet
- KINDRED HEALTHCARE, INC 10-K (Annual Reports) 2009-02-25Document329 pagesKINDRED HEALTHCARE, INC 10-K (Annual Reports) 2009-02-25http://secwatch.comNo ratings yet
- Part List SR-DVM70AG, SR-DVM70EUDocument28 pagesPart List SR-DVM70AG, SR-DVM70EUAndrea BarbadoroNo ratings yet
- Instrumentation and Control Important Questions and AnswersDocument72 pagesInstrumentation and Control Important Questions and AnswersAjay67% (6)
- Partnership Law (Chapter 1 and 2) - ReviewerDocument9 pagesPartnership Law (Chapter 1 and 2) - ReviewerJeanne Marie0% (1)
- ABES Engineering College, Ghaziabad Classroom Photograph: (Ramanujan Block, First Floor)Document21 pagesABES Engineering College, Ghaziabad Classroom Photograph: (Ramanujan Block, First Floor)Avdhesh GuptaNo ratings yet
- Form Ticketing Latihan ContohDocument29 pagesForm Ticketing Latihan ContohASPIN SURYONONo ratings yet
- Job Description Examples - British GasDocument2 pagesJob Description Examples - British GasIonela IftimeNo ratings yet
- Bar Q Salaries Part 2Document5 pagesBar Q Salaries Part 2Brigette DomingoNo ratings yet
- Grammar WorksheetsDocument161 pagesGrammar WorksheetsKhánhNo ratings yet
- Sap On Cloud PlatformDocument2 pagesSap On Cloud PlatformQueen ValleNo ratings yet
- Aml Questionnaire For Smes: CheduleDocument5 pagesAml Questionnaire For Smes: CheduleHannah CokerNo ratings yet
- Unilever Financial PerformanceDocument9 pagesUnilever Financial PerformanceAbdul QayumNo ratings yet
- Juniper M5 M10 DatasheetDocument6 pagesJuniper M5 M10 DatasheetMohammed Ali ZainNo ratings yet