You might also like
- Deresuscitation ARDSDocument28 pagesDeresuscitation ARDSSudaryadiNo ratings yet
- Predicting the Etiology of CLABSI: Bacterial vs Fungal InfectionsDocument19 pagesPredicting the Etiology of CLABSI: Bacterial vs Fungal InfectionssilviNo ratings yet
- Daftar SKDI THT PDFDocument5 pagesDaftar SKDI THT PDFYohanes Daniel Dwiwirya BadawiNo ratings yet
- Jumlah Tetesan Infus MakroDocument2 pagesJumlah Tetesan Infus MakroMamanya Ef Taya ThalitaNo ratings yet
- Soac 2021 First AnnouncementDocument13 pagesSoac 2021 First AnnouncementHendi PrihatnaNo ratings yet
- Dosis Obat Igd PDFDocument3 pagesDosis Obat Igd PDFRiyadila FajarizaNo ratings yet
- Extubation Criteria & Delayed EmergenceDocument3 pagesExtubation Criteria & Delayed EmergenceAnonymous OlS0WZwNo ratings yet
- Daftar Nilai Matrik BA Dan BI T.A. 2017-2018 PDFDocument138 pagesDaftar Nilai Matrik BA Dan BI T.A. 2017-2018 PDFNeni MartiniNo ratings yet
- Calculate Glucose Infusion Rate (GIRDocument9 pagesCalculate Glucose Infusion Rate (GIRarawindahaniastriNo ratings yet
- Circular Gips (Casting)Document14 pagesCircular Gips (Casting)frank runtuboiNo ratings yet
- BAD OBSTETRICAL HISTORY GUIDEDocument34 pagesBAD OBSTETRICAL HISTORY GUIDESagung Ayuska GandhariNo ratings yet
- EmpyemaDocument17 pagesEmpyemadeo_gratias14No ratings yet
- Teknik Anestesi UmumDocument128 pagesTeknik Anestesi UmumAkmalNourNo ratings yet
- Acute Periopertive Pain Management (Sby)Document87 pagesAcute Periopertive Pain Management (Sby)Adam KurniaNo ratings yet
- Hubungan Pengetahuan Bioetika dan Sikap Mahasiswa KedokteranDocument67 pagesHubungan Pengetahuan Bioetika dan Sikap Mahasiswa KedokteranaaaaNo ratings yet
- Farmakologi Obat Analgesik, Anti Piretik & Anti Inflamasi: Andri Tilaqza, M.Farm., AptDocument45 pagesFarmakologi Obat Analgesik, Anti Piretik & Anti Inflamasi: Andri Tilaqza, M.Farm., AptDark BlueNo ratings yet
- CVP Guided Deresuscitation in Managing Overload in Icu PDFDocument57 pagesCVP Guided Deresuscitation in Managing Overload in Icu PDFJonathan Hamm100% (1)
- Heidi's Epinephrine and Amiodarone Infusion for Edema and Doris' TreatmentDocument13 pagesHeidi's Epinephrine and Amiodarone Infusion for Edema and Doris' TreatmentSavero Evan AbishaNo ratings yet
- Differential Diagnosis of Microcytic Anemia PDFDocument5 pagesDifferential Diagnosis of Microcytic Anemia PDFayms99No ratings yet
- I. Similar To Rounded Abdomen Only Greater. Anticipated in Pregnancy, Also Seen in Obesity, Ascites, and Other Conditions IIDocument3 pagesI. Similar To Rounded Abdomen Only Greater. Anticipated in Pregnancy, Also Seen in Obesity, Ascites, and Other Conditions IIroxanneNo ratings yet
- AnestesiDocument59 pagesAnestesiJeffrey EkaNo ratings yet
- Interna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityDocument46 pagesInterna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityErni JawaNo ratings yet
- Patogenesis Dan Patofisiologi Carcinoma Mammae: Reproduc. Factors Lifesyle FactorsDocument4 pagesPatogenesis Dan Patofisiologi Carcinoma Mammae: Reproduc. Factors Lifesyle FactorsStefanus SanNo ratings yet
- Klasifikasi Tumor Paru Secara Histologis Menurut WHO Tahun 2015Document3 pagesKlasifikasi Tumor Paru Secara Histologis Menurut WHO Tahun 2015lindaNo ratings yet
- Sarawak Thromboprophylaxis Risk Assessment Form: NAME: HOSPITAL: Risk Factors: Tick Score AntenatalDocument2 pagesSarawak Thromboprophylaxis Risk Assessment Form: NAME: HOSPITAL: Risk Factors: Tick Score AntenatalTan Chin AunNo ratings yet
- Prehospital Emergency Cardiac Care for STEMI PatientsDocument100 pagesPrehospital Emergency Cardiac Care for STEMI PatientstammypusphitarNo ratings yet
- Integrated Emergency and Disaster Management System in DIYDocument49 pagesIntegrated Emergency and Disaster Management System in DIYHari Mas KuncoroNo ratings yet
- Abnormal Chest FindingsDocument5 pagesAbnormal Chest FindingsAbishek Prince100% (1)
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- Congestive Heart Failure (CHF) / Decompensation Cordis Functional Class (DCFCDocument25 pagesCongestive Heart Failure (CHF) / Decompensation Cordis Functional Class (DCFCYUSRIL ZUMADINSYAHNo ratings yet
- Critical AppraisalDocument47 pagesCritical AppraisalNaman KhalidNo ratings yet
- Congenital Adrenal HyperplasiaDocument14 pagesCongenital Adrenal HyperplasiabangkitayuNo ratings yet
- Cme Acs 2. Stemi (Izzah)Document36 pagesCme Acs 2. Stemi (Izzah)Hakimah K. SuhaimiNo ratings yet
- CPC BEDSIDEDocument7 pagesCPC BEDSIDEaji2703No ratings yet
- Basic ECG Arrhythmia IdentificationDocument74 pagesBasic ECG Arrhythmia IdentificationSibro Malisi100% (1)
- PVC Stoelting Coex 1Document29 pagesPVC Stoelting Coex 1Rudy SiahaanNo ratings yet
- Scientific Communication Medical Information & Clinical ResearchDocument49 pagesScientific Communication Medical Information & Clinical ResearchErick Rangga JuniorNo ratings yet
- Journal Reading Muhamad Fakhri PPDS JantungDocument24 pagesJournal Reading Muhamad Fakhri PPDS JantungLycka AkaishaNo ratings yet
- PratikPatel - Duodenal AtresiaDocument1 pagePratikPatel - Duodenal AtresiaIkhlasia Amali MahzumNo ratings yet
- RozerplastyDocument4 pagesRozerplastyLutfi Aulia RahmanNo ratings yet
- Osteoartritis: Dr. Dewi Nur Fiana.,Sp - KFRDocument28 pagesOsteoartritis: Dr. Dewi Nur Fiana.,Sp - KFRgita cahayaNo ratings yet
- MANAGEMENT ACUTE ISCHEMIC STROKE (Simpo rTPA RSHS) - LisdaDocument63 pagesMANAGEMENT ACUTE ISCHEMIC STROKE (Simpo rTPA RSHS) - LisdadianNo ratings yet
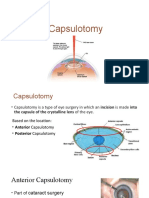
- CapsulotomyDocument15 pagesCapsulotomyAdrian PearlNo ratings yet
- Burat-Buret Echo Romi Revised PDFDocument2 pagesBurat-Buret Echo Romi Revised PDFAsma.denmiNo ratings yet
- Konas Perdatin 2019Document66 pagesKonas Perdatin 2019Akreditasi RSPC19No ratings yet
- Kegawatan Respirasi May2016-FkumyDocument62 pagesKegawatan Respirasi May2016-FkumyAgustina Tri P. DNo ratings yet
- Ophthalmic and Physiological Optics Volume 36 Issue 2 2016 (Doi 10.1111/opo.12275) Tauste, Ana Ronda, Elena Molina, María-José Seguí, Mar - Effect of Contact Lens Use On Computer Vision SyndromeDocument8 pagesOphthalmic and Physiological Optics Volume 36 Issue 2 2016 (Doi 10.1111/opo.12275) Tauste, Ana Ronda, Elena Molina, María-José Seguí, Mar - Effect of Contact Lens Use On Computer Vision SyndromeAdhe WagiNo ratings yet
- F.A.S.T.H.U.G: I W. AryabiantaraDocument35 pagesF.A.S.T.H.U.G: I W. Aryabiantaraarnawaiputu60No ratings yet
- Kuliah Extrapyramidal SyndromeDocument50 pagesKuliah Extrapyramidal SyndromePutri Azka RinandaNo ratings yet
- Relationship between surgical duration and shivering in spinal anesthesia patientsDocument9 pagesRelationship between surgical duration and shivering in spinal anesthesia patientsariefNo ratings yet
- Sop Journal ReadingDocument6 pagesSop Journal Readingriki_rdnNo ratings yet
- Tabel Konversi FiO2Document2 pagesTabel Konversi FiO2arie_yuliantoNo ratings yet
- Lapkas PP (STEMI)Document68 pagesLapkas PP (STEMI)KurbulNo ratings yet
- 13 - 266fourniers Gangrene PDFDocument5 pages13 - 266fourniers Gangrene PDFMochamad RizalNo ratings yet
- Dosis Obat Premedikasi: No Golongan Nama Obat Dosis Dewasa (MG) Dosis Anak RuteDocument1 pageDosis Obat Premedikasi: No Golongan Nama Obat Dosis Dewasa (MG) Dosis Anak RuteDenny RamdhanNo ratings yet
- First Year 2019docxDocument262 pagesFirst Year 2019docxCherry100% (1)
- Perioperative Management 1203114432600412 4Document53 pagesPerioperative Management 1203114432600412 4polushkyNo ratings yet
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisFrom EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisRating: 3.5 out of 5 stars3.5/5 (2)
- Algoritmos AHA ACLS AdultoDocument4 pagesAlgoritmos AHA ACLS AdultoChristianFelipePorrasCastroNo ratings yet
- MySAP TipsDocument28 pagesMySAP TipsSyed Nadir Haseeb Bukhari100% (1)
- Postcolonial Reflections On Luke 1Document19 pagesPostcolonial Reflections On Luke 1Vladimir CarlanNo ratings yet
- Julia Donaldson Reading Comprehension QuestionsDocument18 pagesJulia Donaldson Reading Comprehension QuestionsJasminaNo ratings yet
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlDocument25 pagesFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04No ratings yet
- Bikoko v. Ampco System Parking - Document No. 6Document2 pagesBikoko v. Ampco System Parking - Document No. 6Justia.comNo ratings yet
- Chopin S Polish BalladeDocument214 pagesChopin S Polish BalladeSoni Petrovski86% (7)
- "Tour of Herefordshire" QuizDocument1 page"Tour of Herefordshire" QuizThomas PowellNo ratings yet
- CTET 2012 English Question Paper with Key & ExplanationsDocument7 pagesCTET 2012 English Question Paper with Key & ExplanationsSureshkumaryadavNo ratings yet
- Types of NounsDocument7 pagesTypes of NounsRegine Fe VallespinNo ratings yet
- Integrated Communications Systems Modeling: A Model-Based Engineering ApproachDocument5 pagesIntegrated Communications Systems Modeling: A Model-Based Engineering ApproachRaghavan MuralidharanNo ratings yet
- Esen Learner'S Feedback Formlearner'S Feedback FormDocument4 pagesEsen Learner'S Feedback Formlearner'S Feedback FormClarenzNo ratings yet
- Chapter 9 Stresses in A Soil MassDocument10 pagesChapter 9 Stresses in A Soil MassJefrey DeleonNo ratings yet
- Nutrition ThesisDocument4 pagesNutrition ThesisPaperWritingServiceCollegeUK100% (1)
- PA ToolDocument42 pagesPA ToolShara Lailanie A. AzisNo ratings yet
- SAT EssayDocument1 pageSAT EssayBhavye GuptaNo ratings yet
- Abraham, J. (2008) Are Girls Necessary. Lesbian Writings and Modern Histories PDFDocument240 pagesAbraham, J. (2008) Are Girls Necessary. Lesbian Writings and Modern Histories PDFMarc Jiménez MarzoNo ratings yet
- Paleoclimate Labels of Late Quaternary, Southern Tamil NaduDocument1 pagePaleoclimate Labels of Late Quaternary, Southern Tamil NaduDr.Thrivikramji.K.P.No ratings yet
- Doc-20240208-Wa0003 240208 012035Document7 pagesDoc-20240208-Wa0003 240208 012035anshulthestylorider2No ratings yet
- Skills Workbook: Unit 6Document90 pagesSkills Workbook: Unit 6Rivka Share100% (1)
- Cement Evaluation GuidelinesDocument164 pagesCement Evaluation GuidelinesSaid Nahum Montes CarballoNo ratings yet
- Happy: D.R. ® 2020 Organización Harmon Hall, A.C. 1Document7 pagesHappy: D.R. ® 2020 Organización Harmon Hall, A.C. 1Omar AlfaroNo ratings yet
- Promise To MarryDocument35 pagesPromise To MarryHAR PREET KAUR A P RAJINDAR SINGHNo ratings yet
- IQRA University Sample PaperDocument9 pagesIQRA University Sample PaperFaryal Mughal100% (1)
- Clinically Important EnzymesDocument29 pagesClinically Important Enzymesonnumilla49No ratings yet
- Answers To Problem Sets: How Much Should A Corporation Borrow?Document8 pagesAnswers To Problem Sets: How Much Should A Corporation Borrow?priyanka GayathriNo ratings yet
- Alarm Viewer Activex Control in The Same Screen With Device WizarDocument2 pagesAlarm Viewer Activex Control in The Same Screen With Device Wizarhassan karimiNo ratings yet
- How To Do Eyebrows - A Style Guide For Perfect EyebrowsDocument12 pagesHow To Do Eyebrows - A Style Guide For Perfect EyebrowsnatasyaNo ratings yet
- Market Basket AnalysisDocument12 pagesMarket Basket AnalysisRohit SinghNo ratings yet
- Ethical and Legal Issues in Mental Health NursingDocument18 pagesEthical and Legal Issues in Mental Health NursingUdaya Sree80% (5)
- ElectrocoagulationDocument31 pagesElectrocoagulationMarineil Gomez100% (1)