You might also like
- MFD Part 2 Exam Held in JUST, Jordan On 12-2013Document2 pagesMFD Part 2 Exam Held in JUST, Jordan On 12-2013sohaib197No ratings yet
- Clinical Cases in Restorative and Reconstructive DentistryFrom EverandClinical Cases in Restorative and Reconstructive DentistryRating: 5 out of 5 stars5/5 (1)
- Questions 1 - 100Document15 pagesQuestions 1 - 100Vicky Cezar Villanueva50% (2)
- Avoiding and Treating Dental Complications: Best Practices in DentistryFrom EverandAvoiding and Treating Dental Complications: Best Practices in DentistryDeborah A. TermeieNo ratings yet
- MFD Part 2Document6 pagesMFD Part 2sohaib197No ratings yet
- ORE MCQsDocument268 pagesORE MCQspawi18No ratings yet
- PDF Mcqs in Dentistry For Android 201109133336Document65 pagesPDF Mcqs in Dentistry For Android 201109133336Gloria JaisonNo ratings yet
- Final Exam - Guide For Study and Reading LIstDocument2 pagesFinal Exam - Guide For Study and Reading LIsthanaNo ratings yet
- MFD Part2 Pastpapers According To SubjectsDocument255 pagesMFD Part2 Pastpapers According To SubjectsEnea Nastri100% (3)
- MFD II Online Exams 2020Document8 pagesMFD II Online Exams 2020Ameer FadelNo ratings yet
- Endodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarDocument6 pagesEndodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarGunjan GargNo ratings yet
- What Is Root Canal Treatment?Document2 pagesWhat Is Root Canal Treatment?Vishakha SabooNo ratings yet
- A Guide To Succeeding in The Df1 Interview (Sample Pages Only)Document15 pagesA Guide To Succeeding in The Df1 Interview (Sample Pages Only)jaipald9067% (3)
- Viva Questions For MFD Part 2 ConsolidatedDocument34 pagesViva Questions For MFD Part 2 ConsolidatedEnea NastriNo ratings yet
- OSCEs For DentistryDocument3 pagesOSCEs For DentistryMohammed IssaNo ratings yet
- OSCE - Health PromotionDocument13 pagesOSCE - Health PromotionbabukanchaNo ratings yet
- Sample Questions MJDF Part 1 Sample Questions MJDF Part 1Document21 pagesSample Questions MJDF Part 1 Sample Questions MJDF Part 1HarkanNo ratings yet
- Root FracturesDocument9 pagesRoot FracturesAbhilashPadmanabhanNo ratings yet
- Post-Insertion Denture ProblemsDocument10 pagesPost-Insertion Denture ProblemsRahul MahajanNo ratings yet
- Omsb Orthodontic Prometric Text Content and Test ReferencesDocument1 pageOmsb Orthodontic Prometric Text Content and Test ReferencesAli AlyaNo ratings yet
- MJDF Part 1 QuestionsDocument21 pagesMJDF Part 1 QuestionsHabeeb AL-AbsiNo ratings yet
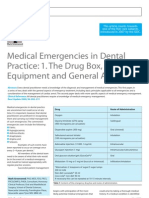
- Medical Emergencies in Dental Practice: 1. The Drug Box, Equipment and General ApproachDocument6 pagesMedical Emergencies in Dental Practice: 1. The Drug Box, Equipment and General ApproachRodelix San Juan Dacanay100% (1)
- MFDS Part1 DetailsDocument2 pagesMFDS Part1 DetailskaizalNo ratings yet
- Endodontics PDFDocument109 pagesEndodontics PDFduracell19No ratings yet
- Australian Dental Journal: Rhinosinusitis in Oral Medicine and DentistryDocument7 pagesAustralian Dental Journal: Rhinosinusitis in Oral Medicine and DentistryVishakha SabooNo ratings yet
- Mother of All Info Orkut VersionDocument19 pagesMother of All Info Orkut VersionApri DhaliwalNo ratings yet
- MFD Exam QuestionsDocument5 pagesMFD Exam QuestionsNidhin VargheseNo ratings yet
- 2013 ABGDsgDocument244 pages2013 ABGDsgteertheshNo ratings yet
- OcclusionDocument14 pagesOcclusionpasser byNo ratings yet
- 31 SJ BDJ 2014 953Document7 pages31 SJ BDJ 2014 953Juan Augusto Fernández TarazonaNo ratings yet
- ABGD Reference ListDocument4 pagesABGD Reference ListFiras Abu SamraNo ratings yet
- Prolonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkDocument5 pagesProlonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkRahulLife'sNo ratings yet
- Modification of Dental Treatment HandoutDocument7 pagesModification of Dental Treatment HandoutnewmexicoomfsNo ratings yet
- The Preliminary Examination For Overseas Trained Dentists, Held by The Australian Dental Council. MCQ Paper II September 05Document6 pagesThe Preliminary Examination For Overseas Trained Dentists, Held by The Australian Dental Council. MCQ Paper II September 05Dr Hufrish Taraporewala100% (8)
- MdsDocument356 pagesMdsARJUN SreenivasNo ratings yet
- New Questions 2015 DentalDocument115 pagesNew Questions 2015 DentalDr-ShadyElOssailyNo ratings yet
- Oral Surgery - QuestionsDocument19 pagesOral Surgery - QuestionskarimelmestekawyNo ratings yet
- Basic Space MaintainersDocument69 pagesBasic Space MaintainersOfier Siki0% (1)
- Overseas Registration Examination Reading ListDocument3 pagesOverseas Registration Examination Reading ListyoNo ratings yet
- Good Occlusal Practice in Advanced Restorative DentistryDocument10 pagesGood Occlusal Practice in Advanced Restorative DentistryMichael XuNo ratings yet
- Treatment Options For Missing Teeth PDFDocument7 pagesTreatment Options For Missing Teeth PDFNajeeb UllahNo ratings yet
- Class VDocument37 pagesClass VyahyaNo ratings yet
- Ellis FracturesDocument40 pagesEllis Fracturespriti adsulNo ratings yet
- A Guide To Managing Tooth Wear The Radboud PhilosphyDocument9 pagesA Guide To Managing Tooth Wear The Radboud PhilosphyNajeeb UllahNo ratings yet
- Canine Impaction Oral SurgeryDocument6 pagesCanine Impaction Oral SurgeryFourthMolar.comNo ratings yet
- Management of Impacted TeethDocument153 pagesManagement of Impacted TeethToma Irina100% (1)
- Twin BlockDocument124 pagesTwin Blockrama deviNo ratings yet
- MFD Last LastDocument56 pagesMFD Last LastFree PizzaNo ratings yet
- Lecture (17) Orthodontic Dentistry .: ساملا نانج د Orthopaedic Appliance in OrthodonticDocument3 pagesLecture (17) Orthodontic Dentistry .: ساملا نانج د Orthopaedic Appliance in Orthodonticاسراء فاضل مصطفى100% (1)
- Endodontic Management of Traumatic InjuriesDocument6 pagesEndodontic Management of Traumatic InjuriesMehwish MunawarNo ratings yet
- Aa 1 MasterRQsDocument93 pagesAa 1 MasterRQsSadhana SabhandasaniNo ratings yet
- Radiology in Pediatric Dentistry 2Document44 pagesRadiology in Pediatric Dentistry 2Aima Cuba100% (1)
- Sorting Out Endodontic Symptoms: ©JK Mitchell, DDS, Med April 2012Document2 pagesSorting Out Endodontic Symptoms: ©JK Mitchell, DDS, Med April 2012sao_tren_troi100% (1)
- Traumatic Injuries of The TeethDocument76 pagesTraumatic Injuries of The TeethJitender ReddyNo ratings yet
- Department of Pedodontics: Submitted By: Shayoni Sen Bds Ivth YearDocument29 pagesDepartment of Pedodontics: Submitted By: Shayoni Sen Bds Ivth YearFarzana ShereenNo ratings yet
- Crown or Bridge Preparation Post Operative InstructionsDocument6 pagesCrown or Bridge Preparation Post Operative InstructionsJyoti RahejaNo ratings yet
- Immediate Dentures - 2Document18 pagesImmediate Dentures - 2Ayad IbrahimNo ratings yet
- 009467gb Helbo User ManualDocument2 pages009467gb Helbo User Manualjuan luisNo ratings yet
- RACDS OSCE - General DentistryDocument16 pagesRACDS OSCE - General DentistryGujapaneni Ravi Kumar90% (10)
- RACDS OSCE - General Practice Part 2Document14 pagesRACDS OSCE - General Practice Part 2juan luisNo ratings yet
- Giuseppe Marchetti Deep Margin Elevation Indirect and Direct Composite Restorations A Clinical Case ViaDocument24 pagesGiuseppe Marchetti Deep Margin Elevation Indirect and Direct Composite Restorations A Clinical Case Viajuan luis100% (1)
- MCQs in DentistryDocument135 pagesMCQs in Dentistrysam4sl98% (84)
- Andrada E. Asmawil CDW 1Q1 PRE K2 DAILY SESSION PLAN 1Document10 pagesAndrada E. Asmawil CDW 1Q1 PRE K2 DAILY SESSION PLAN 1annradaasmawilNo ratings yet
- Unconventional Denture (Autosaved)Document50 pagesUnconventional Denture (Autosaved)Shilpa SomanNo ratings yet
- Anatonical LandmarksDocument5 pagesAnatonical LandmarksSunny RauniyarNo ratings yet
- Penetration DepthDocument8 pagesPenetration DepthSahasraNo ratings yet
- Test Bank For Dental Radiography Principles and Techniques 5th EditionDocument15 pagesTest Bank For Dental Radiography Principles and Techniques 5th Editionhaydencraigpkrczjbgqe100% (25)
- Dentalcariesandpregnantwomen PDFDocument5 pagesDentalcariesandpregnantwomen PDFandreamariefdjNo ratings yet
- Cerabien ZR: For True-To-Life ResultDocument6 pagesCerabien ZR: For True-To-Life ResultOrxan TeymurluNo ratings yet
- Dental Implant MaintenanceDocument7 pagesDental Implant MaintenanceLalaNo ratings yet
- Okd Ohw Report FormDocument25 pagesOkd Ohw Report FormMarilyne S RabangNo ratings yet
- Satelec X Mind Pano CephDocument56 pagesSatelec X Mind Pano CephcacadecabraNo ratings yet
- 5.hand Instruments For Operative Dentistry HadoutsDocument78 pages5.hand Instruments For Operative Dentistry Hadoutssohaib197100% (1)
- Survey of Dentists To Determine Contemporary Use of Endodontic PostsDocument4 pagesSurvey of Dentists To Determine Contemporary Use of Endodontic PostsHector Flores SotoNo ratings yet
- Modified Tunneling TechniqueDocument5 pagesModified Tunneling TechniqueAdam HusniNo ratings yet
- Black 1950 PDFDocument10 pagesBlack 1950 PDFcis freteNo ratings yet
- A New Classification System For The Restoration of Root Filled TeethDocument26 pagesA New Classification System For The Restoration of Root Filled TeethGowtham s100% (1)
- Dental TerminologyDocument3 pagesDental TerminologyJosue MHNo ratings yet
- Mcdonald 2011Document6 pagesMcdonald 2011sinem yıldırımNo ratings yet
- Strategies in Dental Diagnosis and Treatment Planning.Document304 pagesStrategies in Dental Diagnosis and Treatment Planning.docjowin90% (20)
- CHỌN HSG- LỚP 8Document6 pagesCHỌN HSG- LỚP 8Dhāraṇe KusalaNo ratings yet
- Faktor Penentu Keberhasilan Perw OrthoDocument10 pagesFaktor Penentu Keberhasilan Perw OrthoPuan MaharaniNo ratings yet
- ADK GuideDocument21 pagesADK GuideZayd DeenNo ratings yet
- 22.12.2023 Dr. Malhotra Dental Centre Report For Gurpreet SinghDocument1 page22.12.2023 Dr. Malhotra Dental Centre Report For Gurpreet Singhgbj987223No ratings yet
- Morsicatio Buccarum PDFDocument5 pagesMorsicatio Buccarum PDFabhijit8423No ratings yet
- Toothpaste CandyDocument31 pagesToothpaste CandyMd AquibNo ratings yet
- 1 s2.0 S0099239923000067 MainDocument8 pages1 s2.0 S0099239923000067 MainAlejandraNo ratings yet
- Ijerph 18 06796 v2Document24 pagesIjerph 18 06796 v2paolaNo ratings yet
- University of Medicine and Pharmacy at Ho Chi Minh City: English ClassDocument31 pagesUniversity of Medicine and Pharmacy at Ho Chi Minh City: English ClassRiin ĐặngNo ratings yet
- Assessments of PreschoolerDocument8 pagesAssessments of PreschoolerYashoda SatputeNo ratings yet
- Comparison of Obturation Quality in Modified Continuous Wave Compaction, Continuous Wave Compaction, Lateral Compaction and Warm Vertical Compaction TechniquesDocument10 pagesComparison of Obturation Quality in Modified Continuous Wave Compaction, Continuous Wave Compaction, Lateral Compaction and Warm Vertical Compaction TechniquesHachko GiragosyanNo ratings yet
- Act 4 EndoDocument3 pagesAct 4 EndoElizabeth MartinezNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!From EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Rating: 5 out of 5 stars5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)From EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Rating: 4 out of 5 stars4/5 (378)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)