You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Anae 12900Document13 pagesAnae 12900Brenda JaparNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- ParkinsonDocument2 pagesParkinsonFang FangNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- DMDocument3 pagesDMFang FangNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Chronic Kidney Disease: EpidemiologyDocument2 pagesChronic Kidney Disease: EpidemiologyFang FangNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- DementiaDocument4 pagesDementiaFang FangNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Chronic Kidney Disease: EpidemiologyDocument2 pagesChronic Kidney Disease: EpidemiologyFang FangNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Role of Hyperglycemia in Acute StrokeDocument10 pagesThe Role of Hyperglycemia in Acute StrokeFang FangNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Chronic Kidney Disease: EpidemiologyDocument2 pagesChronic Kidney Disease: EpidemiologyFang FangNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Chronic Kidney Disease: EpidemiologyDocument2 pagesChronic Kidney Disease: EpidemiologyFang FangNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- PLENO Pemicu 6 Kelompok 12Document64 pagesPLENO Pemicu 6 Kelompok 12Fang FangNo ratings yet
- THREAT Helps To Identify Epistaxis Patients Requiring Blood TransfusionsDocument6 pagesTHREAT Helps To Identify Epistaxis Patients Requiring Blood TransfusionswitariNo ratings yet
- THREAT Helps To Identify Epistaxis Patients Requiring Blood TransfusionsDocument6 pagesTHREAT Helps To Identify Epistaxis Patients Requiring Blood TransfusionswitariNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Toronto Notes Nephrology 2015 33Document1 pageToronto Notes Nephrology 2015 33JUSASBNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Parts of The Human HeartDocument4 pagesParts of The Human HeartKearly Joy VictorioNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Fisiologi Pengaturan Tekanan Darah SILBERNAGL 2Document6 pagesFisiologi Pengaturan Tekanan Darah SILBERNAGL 221701101016 - Juliana Ayu NugrahaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 'Learner's Activity Sheet Assessment Checklist: Third Quarter - Week 2Document12 pages'Learner's Activity Sheet Assessment Checklist: Third Quarter - Week 2Kareena Ameenah BasmanNo ratings yet
- Budd Chiari Syndrome: by DR - Jino JustinDocument29 pagesBudd Chiari Syndrome: by DR - Jino JustinAjeet LohanaNo ratings yet
- MCQDocument20 pagesMCQanuj sharma100% (2)
- Development of Branchial ArchesDocument4 pagesDevelopment of Branchial ArchesFidz LiankoNo ratings yet
- Urinary Tract Infection (UTI)Document6 pagesUrinary Tract Infection (UTI)Anonymous iG0DCOfNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- AVIATION Flight Physiology: - Kirk Michael WebsterDocument56 pagesAVIATION Flight Physiology: - Kirk Michael WebsterabriowaisNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Depart. Farmakologi Dan Terapeutik: Universitas Sumatera Utara-MedanDocument19 pagesDepart. Farmakologi Dan Terapeutik: Universitas Sumatera Utara-MedanMasyithah TetaNo ratings yet
- ELS - Q2 - Module 7 - Organ Systems of Representative Animals - V2Document22 pagesELS - Q2 - Module 7 - Organ Systems of Representative Animals - V2Alyza Joy Ramirez100% (6)
- MCQ InternalDocument21 pagesMCQ InternalKowsalya SelvarajNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- 15b - Digestive System Anatomy and Physiology SeriesDocument100 pages15b - Digestive System Anatomy and Physiology SeriesNickson OnchokaNo ratings yet
- The artery most likely to be eroded in perforation of the posterior wall of the first part of the duodenum is the superior pancreaticoduodenal artery. It is a branch of the gastroduodenal arteryDocument33 pagesThe artery most likely to be eroded in perforation of the posterior wall of the first part of the duodenum is the superior pancreaticoduodenal artery. It is a branch of the gastroduodenal arteryWahida Amalin Ab RazakNo ratings yet
- Grossing, Staging, and Reporting: An Integrated Manual of Modern Surgical PathologyDocument6 pagesGrossing, Staging, and Reporting: An Integrated Manual of Modern Surgical PathologySOUMYA DEYNo ratings yet
- The Integumentary System: Powerpoint Lecture Slides Prepared by Meg Flemming Austin Community CollegeDocument62 pagesThe Integumentary System: Powerpoint Lecture Slides Prepared by Meg Flemming Austin Community CollegetanarNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Abdomen: Radiology RevisionDocument11 pagesAbdomen: Radiology RevisionhimaniNo ratings yet
- The Lympho Glandular and Intugmentary System: Presenter: Abdurke Dido - Physician (MD) May 22,2011Document62 pagesThe Lympho Glandular and Intugmentary System: Presenter: Abdurke Dido - Physician (MD) May 22,2011Worku KifleNo ratings yet
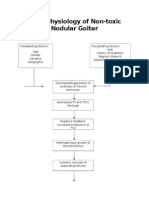
- Pathophysiology of Nontoxic Nodular GoiterDocument2 pagesPathophysiology of Nontoxic Nodular GoiterJan Jewey80% (10)
- Chapter 06Document47 pagesChapter 06gayathmipereraNo ratings yet
- Insuficiencia Renal CrónicaDocument12 pagesInsuficiencia Renal CrónicaJULIO ALONZO UGAZ ABANTONo ratings yet
- PEDI GENITOURINARYDocument7 pagesPEDI GENITOURINARYcayla mae carlosNo ratings yet
- SchistosomiasisDocument92 pagesSchistosomiasisIvan Juan75% (4)
- Chamber One-The Neuro Chemistry of Sex-Level 2Document9 pagesChamber One-The Neuro Chemistry of Sex-Level 2Atyeb Ba Atum Re100% (1)
- 10 - Heart & Great Vessels (FF)Document72 pages10 - Heart & Great Vessels (FF)checkmateNo ratings yet
- Comparative IN: Anatomy of The Stomach Mammalian HerbivoresDocument11 pagesComparative IN: Anatomy of The Stomach Mammalian HerbivoresemeredinNo ratings yet
- sIM3 - Complement System - 22Document37 pagessIM3 - Complement System - 22Brian LeungNo ratings yet
- Brain FactsDocument71 pagesBrain FactsDavid Wang100% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pig Heart and Lung Dissection ProcedureDocument2 pagesPig Heart and Lung Dissection ProcedurelchamblessNo ratings yet
- Practice MCQ Auditory Vestibular SystemsDocument3 pagesPractice MCQ Auditory Vestibular SystemsMawj MandwieNo ratings yet